
A Medical Reversal You May not Have Heard Of
Things are pretty quiet in the summer so let's go back to an old-school medical reversal in electrophysiology. One I lived through. If you like trials you will like this story

The implantable cardioverter-defibrillator (ICD) became popular around the turn of the century after two large seminal trials found large mortality benefits in patients who had heart failure with reduced ejection fraction. Before MADIT II and SCD-HeFT, the ICD was used only in patients who had survived cardiac arrest. These two trials enrolled heart failure patients who had never had an event—so called primary prevention.
Basics:
ICDs work because a lead in the right ventricle senses ventricular tachycardia and then the device charges and delivers either a shock or run of rapid pacing (anti-tachycardia pacing) to terminate the VT. The lead that senses is also used to deliver therapy.
The Achilles heel of these devices are inappropriate therapies, which are terrible because they can cause a) pain and distress, b) induction of malignant arrhythmias and c) have a strong association with increased mortality.
You might wonder how inappropriate therapies occur. The problem happens because the ICD is basically a heart rate counter. If the RV lead senses a rate greater than the (programmable) VT cutoff rate then the ICD delivers VT therapy.
In real life, many non-VT arrhythmias can cause high rates. Things like sinus tachycardia from vigorous exercise, atrial fibrillation, supraventricular tachycardia and even oversensing. Oversensing deserves mention because if the t-wave is sensed, a pulse of 90 beats per minute is sensed as 180 bpm and patients get shocks while wide awake.
It should also be noted that in those early years of the ICD, most doctors believed that ICD settings had to be strict and therapies needed to be delivered as rapidly as possible. ICDs were therefore programmed to act in less than 2.5 seconds, usually for rates > 165 bpm. The faster VT was stopped the better.
Enter the MADIT RIT trial.

Led by the late Author Moss and his team in Rochester, NY, the authors randomized 1500 patients with a primary prevention ICD to one of three programming configurations. This was a large international trial conducted in 98 centers in 6 countries.
Conventional therapy: treat at ≥170 bpm with a 2.5-second delay (standard of the era)
High-rate therapy: treat only at ≥200 bpm with a 2.5-second delay
Delayed therapy: treat with a 60-second delay at 170 to 199 beats per minute, a 12-second delay at 200 to 249 beats per minute, and a 2.5-second delay at ≥250 beats per minute
The primary endpoint of the trial was the first occurrence of inappropriate therapy, defined as antitachycardia pacing or shock delivered for non-VT tachycardia. Two secondary endpoints included all-cause mortality and first episode of syncope (fainting).
The results shocked the EP community
Here is a KM plot of the obviously positive results. Both the “permissive” programming arms (high-rate or delayed therapy) resulted in substantial reductions in the rate of inappropriate shocks.
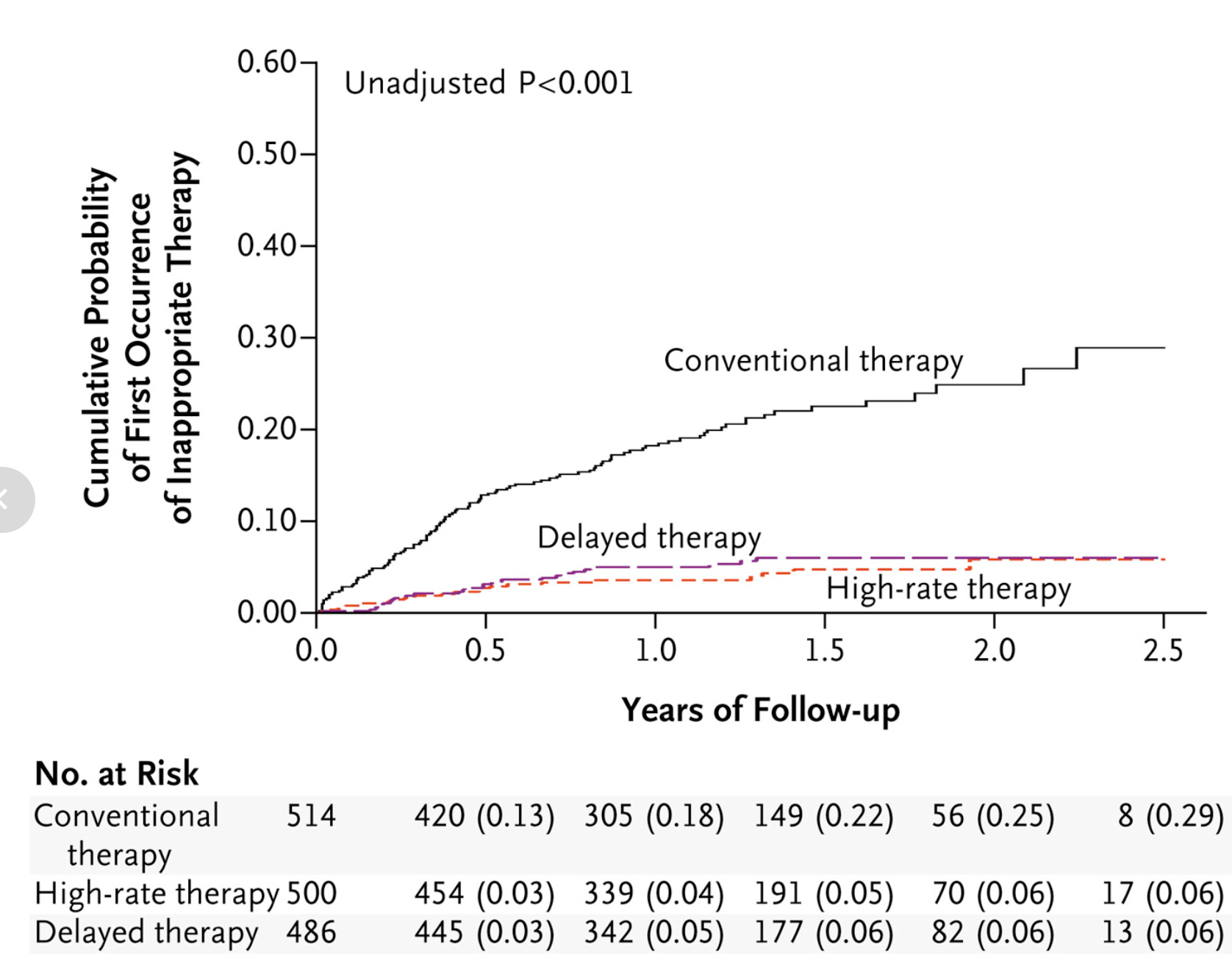
The actual rates of first inappropriate therapy occurred in 105 of 514 patients (20%) in the conventional therapy arm vs 21 of 500 patients (4%) in the high-rate therapy arm vs 26 of 486 patients (5%) in the delayed therapy arm. So the absolute risk reduction was in the range of 15% or an NNT of 7. These were highly statistically significant.
One super-interesting observation was that the two permissive arms also reduced appropriate therapies, from 22% in the conventional arm to 9% and 6% in the high-rate and delayed therapy arms, respectively.
All-cause mortality was reduced by 55% with high-rate programming (p=0.01) and 44% with delayed programming (p=0.06). This was a secondary endpoint, and the death numbers were small (34 vs. 16 vs. 21).
Crucially, syncope rates were identical across all three groups, meaning the more conservative programming did not leave patients unprotected.
Comments
This was a major medical reversal because pre-trial consensus held that one not mess around with VT. A handful of nonrandom studies had suggested permissive programming might be ok, but these had not changed minds.
This well-designed trial provided definitive results. The reduction of inappropriate therapies was clinically important (NNT 7) and statistically robust. Not only was there not a signal of harm, mortality was actually reduced, though the numbers of deaths were small and the signal was statistically somewhat fragile.
Supporting the lack of harm were the identical rates of syncope. In other words, waiting longer—up to 60 seconds—to treat VT, did not increase the rate of syncope.
The reason for the reduction in inappropriate therapy was obvious: supraventricular tachycardias and AF occur in this range, and waiting longer or having a higher rate reduces therapy for these non-VT arrhythmias.
The reason for the mortality reduction is less clear. First, it could have been statistical noise, but if it was a real signal, it may be that the reduction in all (appropriate and inappropriate) therapies was more beneficial than we had thought. Antitachycardia pacing (painless termination of VT with overdrive pacing) can sometimes accelerate the VT. What’s more we also believe that shocks have a detrimental effect on the heart.
MADIT RIT reversed a decade of expert opinion. It affirmed a less-is-more approach to ICD therapy. And remains the standard programming to this day.
Notably, MADIT RIT is an example of an industry-sponsored trial that actually sought an answer to an important clinical question rather than being a marketing exercise.
Everyone involved deserves congratulations. And it’s worth looking back at these examples of medical science done well. Without randomization we may still be programming ICDs in a harmful way.
Great article. Well written.