
A review of the newly approved novel non-opioid pain reliever suzetrigine (Journavx)
It wasn't easy but I tried to summarize the evidence for this new medication.

Last week the FDA approved a novel non-opioid pain medication. The drug is called suzetrigine (Journavx).
A Google search brings up news releases from Vertex, and news coverage—which are essentially the same and lacking links to the evidence.
I aimed to provide readers the evidence for this new drug. This was much more difficult to find.
Some things to set out first: I am not a pain specialist; my analysis is one of a Neutral Martian. Second, a new pain medication would serve a huge unmet need, because many people begin opioid addition from a post-op opioid.
Description of the Drug and its mechanism:
Suzetrigine is a selective inhibitor of the voltage-gated sodium channel Nav1.8, which are primarily expressed in peripheral sensory neurons. By blocking Nav1.8, suzetrigine reduces the ability of pain-sensing neurons to generate and transmit pain signals. This mechanism is more targeted than traditional local anesthetics, which block multiple sodium channel subtypes.
It is an oral table given as a loading dose then 50mg every 12 hours for acute pain. Studies show that it does not have opioid-like properties nor does it act on opioid receptors.
Phase 2 Studies
The NEJM published a placebo-controlled Phase-2 (dose-ranging) study of suzetrigine vs placebo and combination tablet of 5 mg hydrocodone/325 acetaminophen (HB/APAP; 5/325 mg every 6 hours).
This is where I introduce the primary endpoint of these studies: the time-weighted sum of the pain-intensity difference (SPID) over the 48-hour period (SPID48). This is derived from the score on the Numeric Pain Rating scale (range 0-10).
During acute pain trials, patients are assessed about 19 times in this two-day period. The differences (from baseline) at each time are summed and weighted to come up the score. Higher numbers mean better pain relief compared to the placebo.
In the Phase-2 study about 300 patients were studied after abdominoplasty and 274 studied after bunionectomy.
In the main analysis the mean difference in the SPID48 between the high-dose suzetrigine and placebo was 37.8 for the abdominoplasty trial and 36.8 for the bunionectomy trial. Both were statistically significant.
Here is a graphical look at the pain reduction vs placebo. It looks pretty modest to me. (7 vs 6; 6 vs 5 and the error bars get close.)

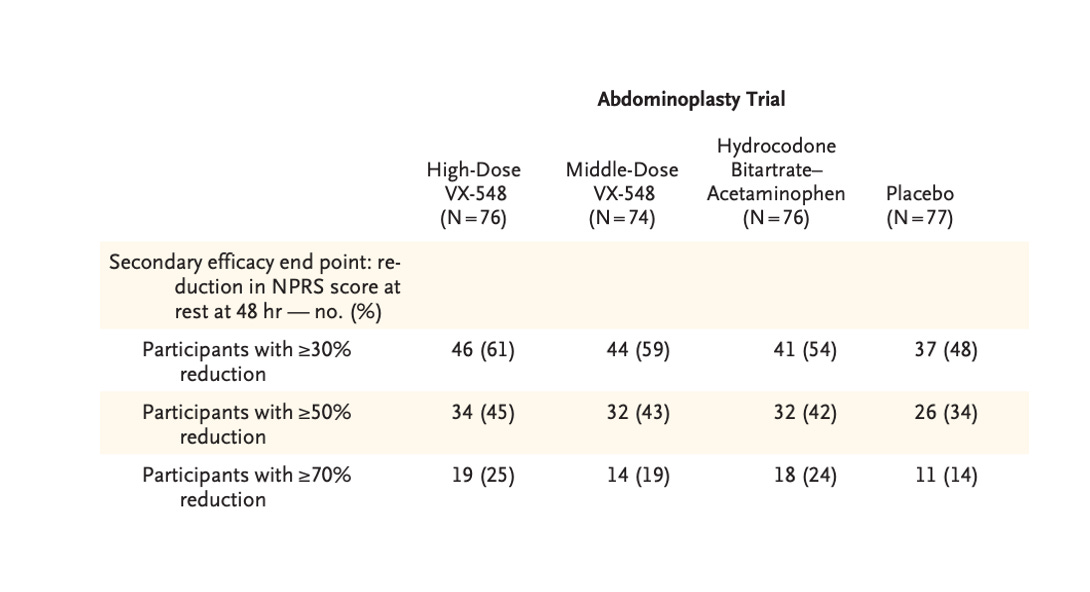
This screen shot shows a reason for caution on efficacy. You can see that the number of patients with >30%, >50% or >70% relief with the high dose drug is not much different from low dose HB/APAP.
Adverse effects were largely similar to placebo, though headache and constipation were slightly higher in the suzetrigine group.
Notable too from the NEJM paper is a heavy industry influence. “The second and third authors and the medical writers were employed by the sponsor, and medical illustrators who were paid by the sponsor.”
Phase 3 Studies
These are not published. They were presented at an anesthesia meeting in October. Here is the link to the abstract.
While we can’t look at the intricacy and nuance of the data, I suspect that FDA reviewers did. I tried but could not find any written summary from FDA.
Here is what I see: The NAVIGATE 1 and 2 trials took a similar form of testing the drug for acute pain following abdominoplasty and bunionectomy. Now there were ≈ 1100 patients in each of the two trials.
Each trial had three arms: suzetrigine, (HB/APAP; 5/325 mg every 6 hours) or placebo.
The primary endpoint was similar—SPID48. Key secondary endpoints were SPID48 for SUZ compared to HB/APAP and time to ≥2-point reduction in NPRS from baseline for SUZ compared to placebo. Safety was assessed as a secondary endpoint.
Results:
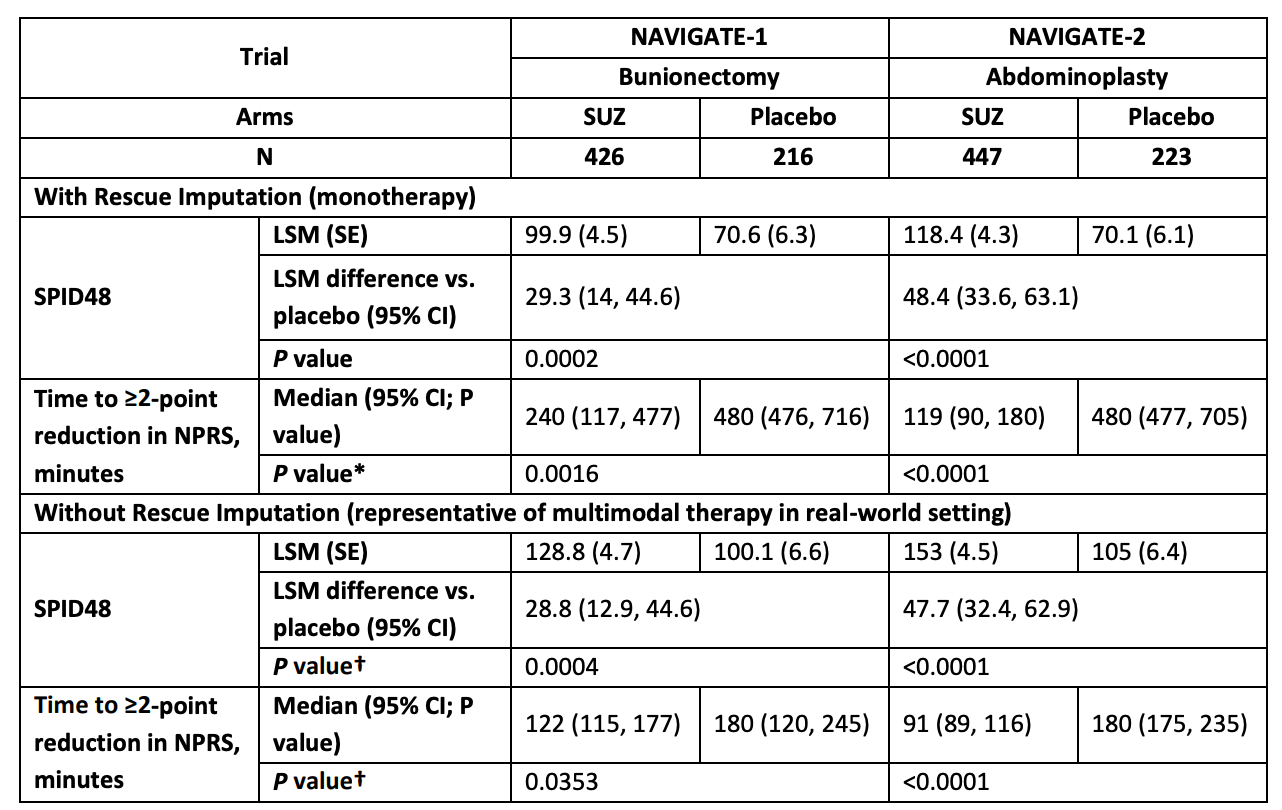
The picture sums the main results.
In both trials, suzetrigine resulted in a statistically significant higher SPID48--29.3 in the bunionectomy trial and 48.4 in the abdominoplasty trial. The time to pain relief greater than 2 points was also favorable in both trials. And it was also significant in the sensitivity analysis using rescue meds.
However, suzetrigine fared no better (even worse in the bunionectomy trial) against low-dose HB/APAP.

The abstract report showed no significant adverse effects compared with placebo.
ICER Review
I found an ICER review by a group called the Midwest Comparative Effectiveness Public Advisory Council. “The Midwest CEPAC Panel is an independent committee of medical evidence experts from across Midwest, with a mix of practicing clinicians, methodologists, and leaders in patient engagement and advocacy.”
They did a systematic review and network meta-analysis of pain relief meds. Note a network meta-analysis tries to compare drugs that have not been directly compared. See the image:

Here is a summary of their findings of the network meta-analysis:
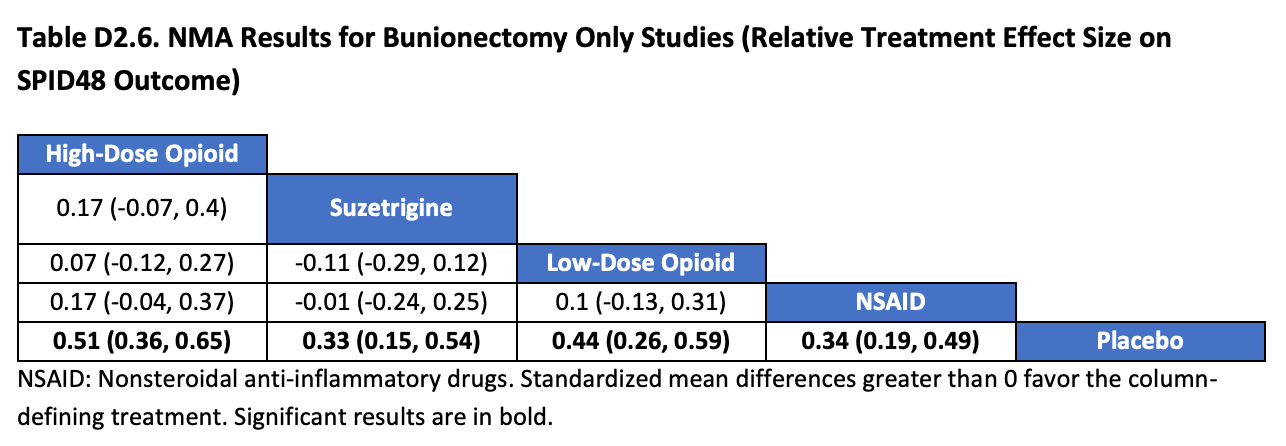
On the bottom row, you can see that NSAIDs, low-dose opioid, suzetrigine and high-dose opioid all reduce SPID48 by similar amounts vs placebo.
On the second row, with NSAID as the comparator, neither opioid dose nor suzetrigine reduce SPID48. (Though remember these are not all direct comparisons).
On the third row, we already know that suzetrigine was no better than low-dose opioid.
