
A Surprising Look at the Evidence for Beta-Blockers After MI
There are few more accepted practices in cardiology than giving beta-blockers after myocardial infarction. The supporting evidence, however, made me stop and think.

Let’s go back in time and look at the evidence behind one of cardiology’s most accepted practices. You might be surprised. I surely was.
The practice is the use of beta-blockers after myocardial infarction (MI). I can’t recall seeing a recent post-MI patient who was not on a beta-blocker. It’s a quality measure now. Doctors and hospitals incur penalties if a patient with an MI is not on a beta-blocker—unless there is a darn good reason put down in the chart.
This discussion also offers me a chance to point learners to a new effort I am doing with my friends Drs. Andrew Foy and Muhammed Ruzieh over at Cardiology Trials Substack.

Our project is to write a textbook of cardiology trials. A place where a learner can go to look up the seminal trials that established modern day cardiology practice. One-page summaries, in book form, outlined by topic. We were about a third done, when the idea struck to write this book on Substack. Our first posts were on two of the early beta-blocker trials—B-HAT and ISIS 1. Boy did these trials surprise me.
BHAT
JAMA published the BHAT trial in 1982—an era before thrombolysis was common. The idea to use beta-blockers stemmed from the drugs ability to reduce oxygen demand through lower heart rate and decreased contractility. That was an important factor for MI therapy in that era because many of the complications of MI were due to excess wall stress from an occluded artery.
BHAT screened more than 16,000 patients with MI but only randomized about one in five of these patients to either propranolol or placebo. Of the nearly 3800 patients screened, most were young white men. Average age 55 years.
Here comes a key feature: patients were randomized 5-21 days after the hospital admission. The average length of stay for MI in 1980 was 14 days. Then, patients were closely monitored, and study drugs vs placebo were increased only if patients tolerated the drug.
The results were that at 2 years, 10.5% of the placebo group died vs 7% in the propranolol arm. This 3% absolute risk reduction was highly statistically significant. And it was driven by lower rates of cardiac death.

The main takeaway from BHAT was that, yes, oral propranolol given in very careful fashion, on or after day 5, to a highly selected group of patients after MI, in the 1980s, reduced death.
ISIS 1
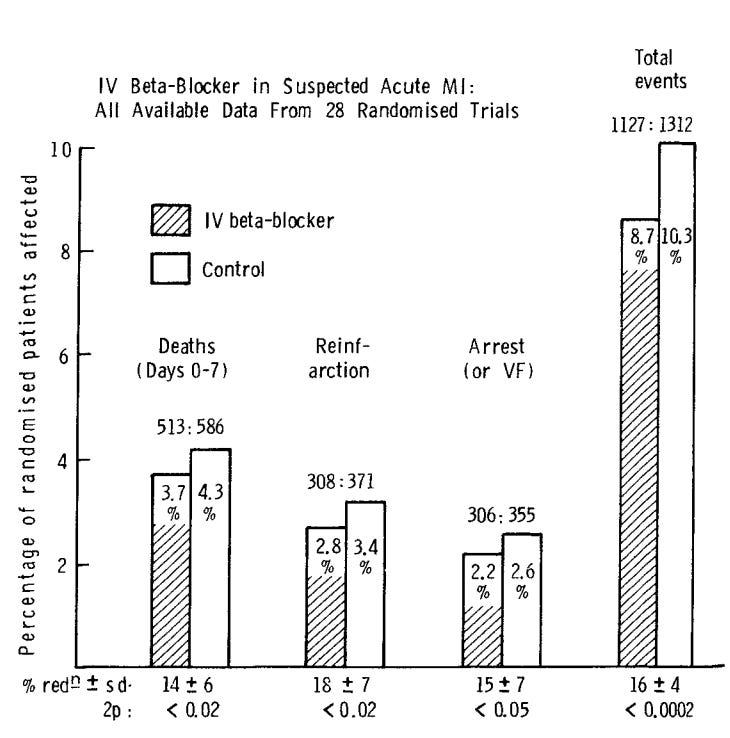
The Lancet journal published ISIS 1 in 1986. This trial tested the use of early IV beta-blocker (atenolol) in patients with MI. Instead of starting oral beta-blocker many days after MI in BHAT, ISIS1 tested immediate use of IV beta-blocker.
The trial enrolled a broad patient group of suspected MI. ISIS 1 intended to be a more pragmatic trial than BHAT. Once again, patients were mostly young males (average age 59 years). Importantly, the mean SBP and BP at entry were robust at 145 mmHg and 79 beats per minute.
Five mg of IV atenolol was given immediately and repeated again in 10 minutes if the HR and BP were ok. If after another 10 minutes, the HR > 40 bpm, oral atenolol 50 mg was given. Twelve hours later another 50 mg of oral atenolol was given. And if possible based on HR and BP, the patient received 100 mg daily of atenolol.
The control group was standard of care. No placebo. Beta-blockers were to be avoided unless thought to be indicated.
About 16,000 patients were randomized from more than 200 hospitals. More than 90% of patients in the active arm received at least one dose of IV atenolol. More than one in four patients, however, had to have a dose reduction or stoppage of atenolol.
During the treatment period (0-7 days), 3.9% of patients in atenolol group had the primary endpoint of vascular death vs 4.6% om the control arm. This 0.7% absolute risk reduction met statistical significance.
At one year, the atenolol group maintained this small absolute risk reduction in both vascular and all-cause death. (Vascular death -- 10.3% vs 11.6%; all-cause death - 10.8% vs 11.9%). Note that nearly all the deaths in ISIS 1 were cardiac, which tells you that this was a pretty healthy patient group.
One really curious subgroup was the male-female group. While men accounted for the majority of patients (77%) and most of the vascular deaths (65%) in the first week, there was no signal of benefit from atenolol (3.5 vs 3.7%). But in women, who accounted for only 23% of the total patients and only one-third of vascular deaths seemed to garner big benefits from treatment (5.2 vs 7.5%). I don’t why this is. And the authors did not mention it.
One other highly relevant subgroup was that patients with hemodynamic instability (lower BP and higher HR) had higher rates of vascular death, but there was no benefit from beta-blocker. In fact, in this subgroup, vascular death was higher in the atenolol arm.
The key takeaways from ISIS 1 was that early IV beta-blocker followed by oral beta-blocker did reduce vascular and all-cause mortality, but the absolute differences were small (about 1% or an NNT ≈ 100). Sicker patients with unstable presentations got no benefit.
Putting the trials together and thinking about MIs in 2024:
These were—basically—the seminal trials that established beta-blockers after MI.
BHAT is hardly applicable today because the average time to starting beta-blocker was 14 days. Almost zero post-MI patients today stay in the hospital more than 5 days.
BHAT also screened many more patients than it enrolled. And it was done during an era when patients suffered severe cardiac damage from a persistently closed coronary artery. That is totally different than now, where patients nearly always have early opening of the closed coronary during an MI.
As for IV beta-blocker, ISIS randomized patients who were quite stable (note the average HR and BPs were well within normal.) The trial had a higher death rate than BHAT but the degree of risk reduction was less than BHAT. ISIS also found a signal of harm from using beta-blockers in sicker patients.
What surprised me in looking closely at these trials is that my previous view that beta-blockers were hugely important really was not grounded in strong evidence.
Especially now that MI therapy has changed so drastically. I never knew that BHAT started oral beta-blockers on day 14!
Fortunately, there are many ongoing trials re-looking at the use of beta-blockers after MI. I strongly suspect that these trials will reverse a common practice. This story speaks to the idea that many trials should have an expiration date.
Foy, Ruzieh and I believe there is great value in studying the seminal trials. This first look surely supports that view. Cardiology Trials Substack will also include a podcast.
John,
As a retired Family doc, I really appreciate your look at established practices that have taken on a kind of evangelical reverence. In medicine nothing, nothing, is sacred! Or should be.
Love your intellectual honesty. Please keep on keepin' on! mm
Our STS quality requirements also use beta blockers even though data based on huge STS database shows no advantage. Like the AFib quality parameters.