
Breaking News: I found a good observational study
Diltiazem vs metoprolol in patients with AF on direct acting oral anticoagulants. Is there a difference? Is it correlation or causation? Does it matter?

The Annals of Internal Medicine has published a darn good observational comparison study. The bonus is that it addresses one of Medicine’s most underrated problems: drug-drug interactions.
Millions of patients have atrial fibrillation. A large fraction of these patients take two classes of drugs—a direct acting oral anticoagulant (DOAC), usually rivaroxaban or apixaban, and a heart rate controlling drug diltiazem or metoprolol.
It turns out that these two drugs can interact with each other.
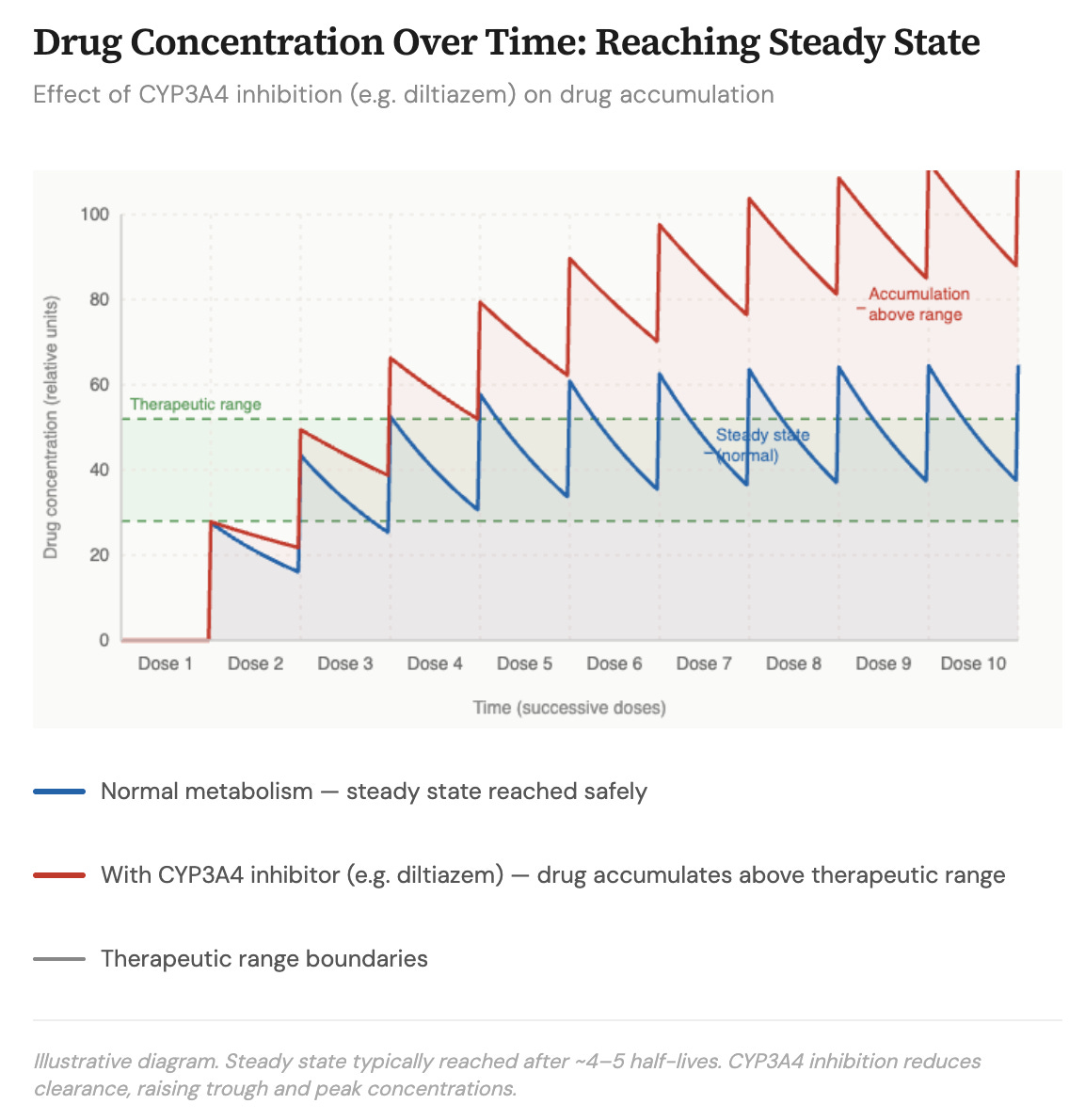
Now we have to get into some minor details about how the body deals with medicines. We are said to metabolize a drug. This means that the amount of drug coming in is balanced by the body’s clearance of the drug. Clearance can be by chemically altering the drug or simply excreting it in the urine.
If we did not clear (or metabolize) drugs, they would just build up to toxic levels. Instead, drug metabolism allows the body to get to steady state where the amount going in is similar to the amount being cleared. A steady state of a drug level is thus maintained.
It turns out that both rivaroxaban and apixaban depend on chemical processes (in the liver, gut wall and kidneys) to be metabolized and cleared. [The enzymes are called cytochrome P450 3A4 (CYP3A4) and P-glycoprotein (P-gp)]. And the drug diltiazem is a potent inhibitor of these processes. Metoprolol, on the other hand, does not inhibit these processes.
You can see the potential clinical problem, which could affect millions of people because AF and these drug combinations are so common. If diltiazem resulted in higher levels of oral anticoagulant, then there may be more bleeding in patients who take diltiazem compared to metoprolol. Claude helped me make this theoretical picture.
The Study
The Vanderbilt team used an insurance database to find adults who were newly starting either apixaban or rivaroxaban. They found about 23,000 patients on one of these anticoagulants who took diltiazem and 85,000 who took metoprolol.
These were not randomized groups. As it is in all non-randomized observational studies, a human clinician decided to use either metoprolol or diltiazem.
The next step is to attempt to balance the two groups. The authors used propensity matching. This resulted in two groups of 23,000 patients who on paper had similar characteristics. The patients were followed for a year.
The primary endpoint of interest was serious bleeding requiring hospital admission, which is available in the database. The authors did some extra analyses, one in particular that was important was a comparison of bleeding events on low vs high doses of diltiazem.
The picture shows the main result.
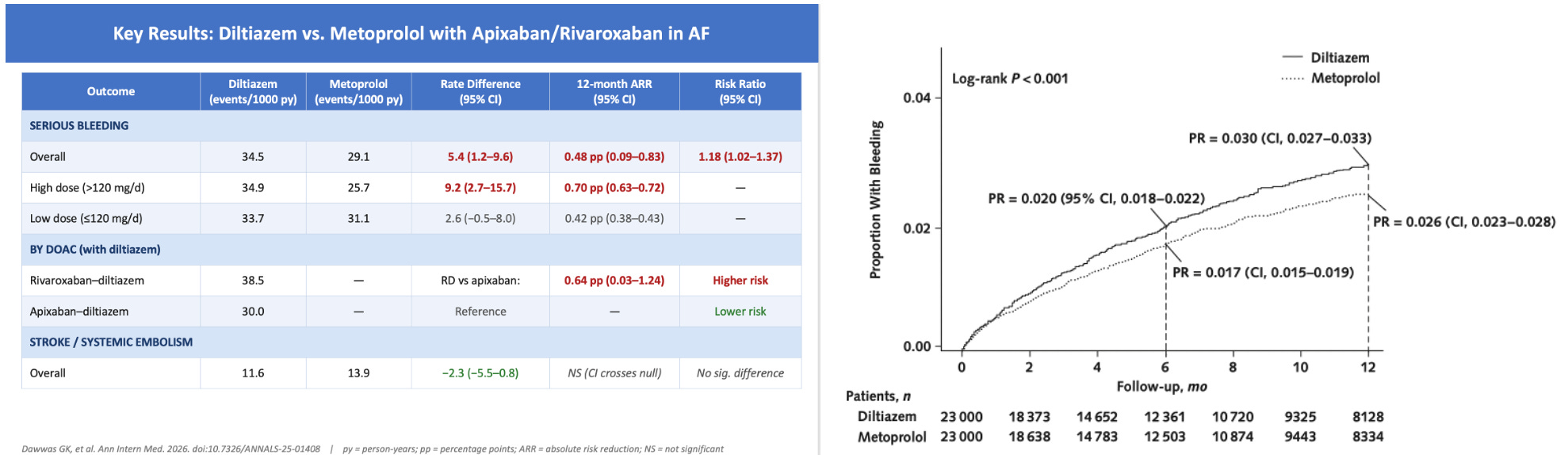
Patients who took diltiazem had an 18% higher rate of bleeding than those on metoprolol. The 95% CI went from 1.02-1.37.
The absolute differences were small. There were 34 vs 29 bleeding events per 1000 patients years. Another way of thinking about that is 0.34 vs vs 0.29 per 100 patient years, which is similar to 0.34% vs 0.29%. That would translate to a number needed to harm of approximately 300 patients using diltiazem over metoprolol.
Comments
The first thing you should think about is whether this association is causal or confounded by other factors, such as, patients on diltiazem were sicker or more apt to bleed.
Residual confounding is always possible in non-random comparisons, but here are four points in favor of true causation rather than correlation.
Point 1: The KM curves do not separate immediately. It takes time (or exposure) to separate. This suggests causation as longer exposure to higher anticoagulant levels should gradually increase bleeding rates.
Point 2: Another suggestion of causation comes from the analysis of diltiazem dose. You’d expect a higher dose of diltiazem to have more blockade of metabolic factors and higher anticoagulant dose. And that would lead to higher rates of bleeding. Indeed, the absolute rate increase of bleeding events was greater in the higher dose diltiazem group. In Bradford Hill causation criteria, this is known as a dose response.
Point 3: There may also be a small clue in the different bleeding rates with rivaroxaban vs apixaban. It turns out that rivaroxaban depends more on CYP3A4-mediated interactions than apixaban. When diltiazem blocks CYP3A4, rivaroxaban levels are likely pushed up more than apixaban levels.
And again, bleeding rates were slightly higher with the rivaroxaban/diltiazem combination than apixaban/diltiazem combination. This was a secondary comparison and confidence intervals barely excluded no effect, so caution is warranted. But it’s directionally consistent with the drug-drug interaction effect.
Point 4: My final proposal that this association is causal stems from experience. To wit, the choice of metoprolol vs diltiazem is often random. The drugs both slow the rate of conduction of AF through the AV node. While we tend to use diltiazem in patients with lung disease, and metoprolol in patients with coronary artery disease, in most cases, whether a person ends up on one or the other is largely random.
Clinical Action
The first clinical take-home is that drug-drug interactions are real. We should be mindful of them. They come in two varieties: this one is called pharmacokinetic, wherein one drug alters the metabolism of another. The other variety is pharmacodynamic wherein two drugs have additive effects. Eg: digoxin and metoprolol interact because they both slow heart rate.
The second take-home is that a diltiazem-DOAC combination probably does increase bleeding vs a metoprolol-DOAC combination. The difference however is tiny. It’s less than 0.5% in absolute terms. WIth a number needed to harm of more than 300, most people on the combination would have no effect.
This absolute risk increase may be significant in a population of hundreds of thousands, but on an individual level, it’s tiny. There are patients who feel worse on beta-blockers. For these patients, diltiazem works well. I don’t see a problem with using the drug combination in an average patient. The one caution here is that this was only a one-year study. The effect size might be larger at 5-10 years.
I might also be more concerned about patients who had inherently higher bleeding risk. Say they were on antiplatelet drug after a coronary stent, or had low platelet count. In these patients, this tiny risk increase could sway me to use metoprolol for rate control.
In sum, this was a nice observational study. It’s not completely definitive but it’s highly suggestive for very small but real effect from a common drug-drug combination.
It stands out as a non-random observational study that gets very close to causal inference. That’s highly unusual. And it underscores the matter of pharmacology, which is underappreciated in clinical medicine.
Thank you. I appreciate these simple “walk me through” explanations of clinical research. Sooner or later I will get it!
Having worked with the authors in Reference 5 on the apixaban clinical pharmacology program from first-in-human until I retired 3 years ago, I can attest to the goodness of this study. It’s spot on and, again, distinguishes apixaban as the DOAC of choice for AF and other indications.