
Chemical Imbalance – Dangerous myth or harmless white lie?
By Abirramy Varatharajan

A couple of weeks ago when Dr. Joanna Moncrieff’s paper on the “serotonin hypothesis” was published in Molecular Psychiatry 1, it hit the news and generated unusual interest for this field. The main finding of this umbrella review, which included over 17 studies (mainly systematic reviews and one large genetic association study), was that serotonin levels were not significantly linked with depression.
This surprised many. People diagnosed with depression felt understandably confused. Since the most commonly prescribed antidepressants (SSRI), act by increasing serotonin levels, a heated debate broke out over their efficacy and need.
Many psychiatrist were quick to counter and stressed the importance of these life-saving drugs. They also reminded us, that we do not need to fully understand the mechanism of action of a drug class for them to be useful. In fact, what seemed like news too many people, was not really news to academic psychiatrists. To understand this we need to dig a little deeper into the history of the “chemical imbalance” theory.
In 1965 Dr. Schildkraut proposed the hypothesis 2 that depression is linked with the levels of certain neurotransmitters in our brain (which later came to known as the “chemical imbalance” theory). His initial focus was on norepinephrine, however soon serotonin was identified as a more promising candidate. At that time there was no evidence to either support or disprove his theory. Researchers soon set out to fill that gap. However decades of research could not find any significant association between the levels of any neurotransmitter and depression. One study in 1974 concluded “The literature reviewed here strongly suggests that the depletion of brain norepinephrine, dopamine or serotonin is in itself not sufficient to account for the development of the clinical syndrome of depression”. 3 Seen in this light, Dr. Moncrieff’s results do not represent brand new information, but rather summarize and solidify what has been known for nearly five decades by now.
Well if this is old news, then why this uproar and why now? What is known to psychiatrists, has not reached the public yet. Studies4 suggest that a majority of people (67%) attribute mental illnesses (as depression) to neurobiological causes (the leading one being the chemical imbalance theory). This number has been increasing since the mid-90’s. Long after it was well established in circles of academic psychiatry that the chemical imbalance theory has no real scientific weight. Instead of correcting this misunderstanding, many psychiatrist in fact encouraged this view. Their reasoning was that a neurobiological explanation for mental illness would decrease stigma and help patient seek out help. According to them, the chemical imbalance theory should not be viewed as a scientific fact but rather as a mental model to better understand the complex pathophysiology of depression. It was a metaphor, if you will.
Well is that true? While studies found that the belief in the chemical imbalance theory increased, no decrease in stigma could be found4. Moreover subscribing to a neurobiological understanding of their disease was associated with prognostic pessimism in people suffering from depression5. People who believed, that they suffered from a condition caused by altered brain chemistry assumed their symptoms to be more fixed and longer lasting, than people that did not hold this belief. However there’s an upside. Subscribing to a neurobiological model generally increases the acceptance for psychiatric treatment4 (in particular medication) and prognostic pessimism can be countered with education about the malleability of the brain’s chemistry (by means such as medication)5. So, even if it doesn’t directly decrease stigma there seems to be some use to this model. It increases the likelihood of people reaching out for help. It also helps people accept medication more easily. After all those are life-saving drugs right? If there is, anything that can be done to help more people take them, then isn’t that in itself good? Even if the science on the matter is standing on rather shaky grounds.
Well do they save lives? As many things in medicine it is complicated. To be clear when I say “saving lives” I will mainly focus on the effect of antidepressants on suicide, since that is what concerns most people while talking about depression. It is not easy to evaluate the effect of antidepressants on suicide since it is (thankfully) a rare event and since people with a high risk of suicide are mostly excluded from randomized trails. What is known, is that there are concerns about increased risk of suicide at the onset of treatment with SSRI. These concerns were first raised in the 90’s. Since then it has been a topic of a heated debate, that is till date far from being settled.
Various meta-analysis and re-analysis of the same data set lead to both confirmatory and contradictory results. While systematic biases such as underreporting and misclassification of suicidal behaviour might lead to an underestimation of the risk. The best available data 6 (meta-analysis of randomized trails) suggests an age dependent relationship with the highest risk in children and adolescents (below the age of 25). This lead the FDA to issues a black box warning in that age group with a recommendation for close monitoring upon starting a treatment regime. Intermediate age groups seem to be not affected in either direction, while there seems a protective effect in the elderly (above 65). Observational data 7 suggest a broader protective effect, however they should be enjoyed with caution, since confounding by indication might play a big role here. A broad protective effect could not be indisputably established in randomized trails. There might be some protective effect in certain age groups; however there are also some risks in other age groups. Overall, it is fair to conclude that SSRI are not primarily life-saving drugs. Their main effect is symptomatic.
So what is their effect then? Evaluating the efficacy of antidepressants is a complex task, going into all the details would go beyond the scope of this essay. Nonetheless, I will try my best to give an overview. Before going straight into the data there are some important biases, that we need to consider, which might lead to an overestimation of the effect of antidepressants. I will mention just a few to give the reader an idea. One important drawback in most trails is the lack of an active placebo. SSRI have some very specific side effects (like dry mouth etc). If the placebo group does not have an active substance mimicking the same side effects, it is fairly easy for participants to guess in which group they are, thus effectively unblinding the trail. Given that the outcomes are highly subjective even little unblinding can have a big impact.
Another important problem are inadequate wash-in periods. Patients that were previously treated with an SSRI are often abruptly switched to placebo, when they enter a trail. Suddenly stopping SSRI is not recommended, since that can produce some unpleasant side effects, quite similar to the symptoms of depression itself. The artefact of these withdrawal symptoms in the placebo group can show the experimental arm in a more favourable light.
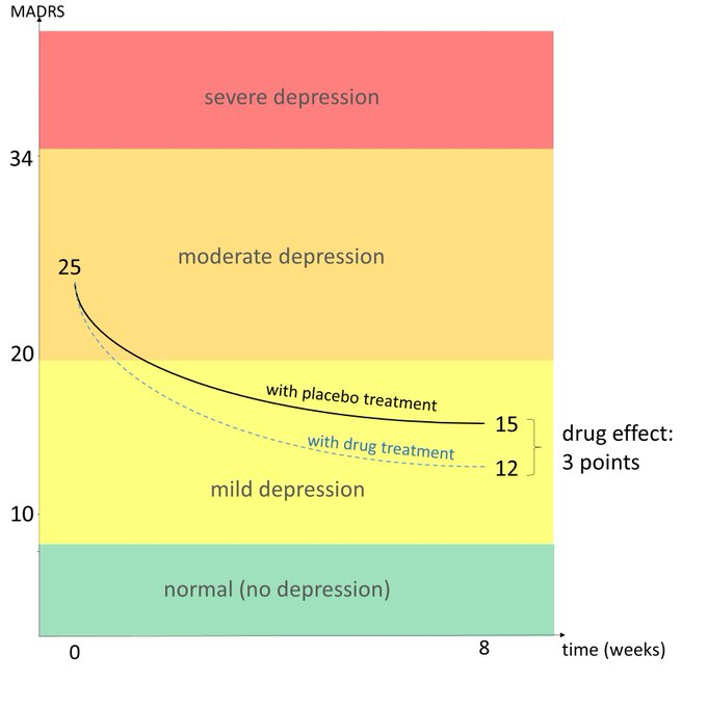
Then there is also publication bias. Pharma firms that are mostly sponsoring these trails are not very keen to publish trails with negative results. Keeping all these caveats in mind, now let us look at the data. The most favourable interpretation of the data 8 suggest that SSRI have a moderate effect on the main symptoms of depression, over a short period of time (measured in weeks). That would be in the range of 3 points difference between placebo and active drug on a 24 point scale. A good way of visualizing this is shown in the picture below (not referring to any particular trail, by @PloederlM).
In summary, we can say that SSRI are drugs with a moderate effect size at best, that might have some protective effect against suicide in some age groups. They certainly are not life-saving miracle drugs. So what are we to do with this information? I do not think it is necessary to advocate for a complete cessation of the use of these drugs. They do have some benefits. Many patients do feel helped by them. However, they are mainly symptomatic drugs and as such, I think the agency to use them should largely lay with the patient. This agency can only be fully asserted if patients are equipped with accurate information. It is important to keep in mind that we are talking about drugs with some serious side effects, such as sexual dysfunction. It is entirely reasonable for a patient to decide that the moderate benefits are not worth the side effects.
I cannot see how convincing anyone with clever metaphors, would be in their best interest. After all, it would never cross any doctor’s mind to use any sophisticated rhetoric to convince his patient suffering from fever to take paracetamol, or convince a sleepless patient with clever metaphors to take his sleeping pills. Why should that be any different when it comes to psychiatric medications? It is my humble opinion that, when it comes to medicine, honesty is the best policy. Clever metaphors and white lies, no matter how well intentioned can never empower patients to make the right choices for themselves. In conclusion, I think it is high time to let the chemical imbalance myth rest and provide patients with more accurate and relevant information.
Abirramy Varatharajan is a Swiss Medical Student
1. Moncrieff, J., Cooper, R.E., Stockmann, T. et al. The serotonin theory of depression: a systematic umbrella review of the evidence. Mol Psychiatry (2022). https://doi.org/10.1038/s41380-022-01661-0
2. Schildkraut, J J. “The catecholamine hypothesis of affective disorders: a review of supporting evidence.” The American journal of psychiatry vol. 122,5 (1965): 509-22. doi:10.1176/ajp.122.5.509
3. Mendels, J, and A Frazer. “Brain biogenic amine depletion and mood.” Archives of general psychiatry vol. 30,4 (1974): 447-51. doi:10.1001/archpsyc.1974.01760100019004
4. Pescosolido, Bernice A et al. “"A disease like any other"? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence.” The American journal of psychiatry vol. 167,11 (2010): 1321-30. doi:10.1176/appi.ajp.2010.09121743
5. Lebowitz, Matthew S et al. “Fixable or fate? Perceptions of the biology of depression.” Journal of consulting and clinical psychology vol. 81,3 (2013): 518-27. doi:10.1037/a0031730
6. Stone, Marc et al. “Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration.” BMJ (Clinical research ed.) vol. 339 b2880. 11 Aug. 2009, doi:10.1136/bmj.b2880
7. Barbui, Corrado et al. “Selective serotonin reuptake inhibitors and risk of suicide: a systematic review of observational studies.” CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne vol. 180,3 (2009): 291-7. doi:10.1503/cmaj.081514
8. Gibbons, Robert D et al. “Benefits from antidepressants: synthesis of 6-week patient-level outcomes from double-blind placebo-controlled randomized trials of fluoxetine and venlafaxine.” Archives of general psychiatry vol. 69,6 (2012): 572-9. doi:10.1001/archgenpsychiatry.2011.2044
 | A guest post by
|
As a clinical psychologist with 40 years of experience, I can attest that the vast majority of depressed patients come to realize that drug treatment has not done them any good, but have trouble ending it because of withdrawal, or what Pharma euphemistically calls "discontinuation syndrome." Ask yourself the simple question: if antidepressants were effective, why would we need a dozen or more of them? Switching to one drug or another is extremely common, and contributes to the myth that biological psychiatrists are "fine tuning" the treatment. In reality, it's all a shell game. My cynicism is born of experience, second-hand, hundreds of times over, as well as reviews of the literature.
Thanks for a very fair and accurate post.
This article is very well written, but the best thing about it is its tone. The humble, thoughtful nature by which the recommendations are conveyed strikes a great balance between clarity without misleading the reader about the uncertainty present in this area. Fauci and the CDC could learn a lot about communications from this article.