
COVID19 Therapeutics & Boosters all need new studies
The current on the ground reality has nothing to do with 2020

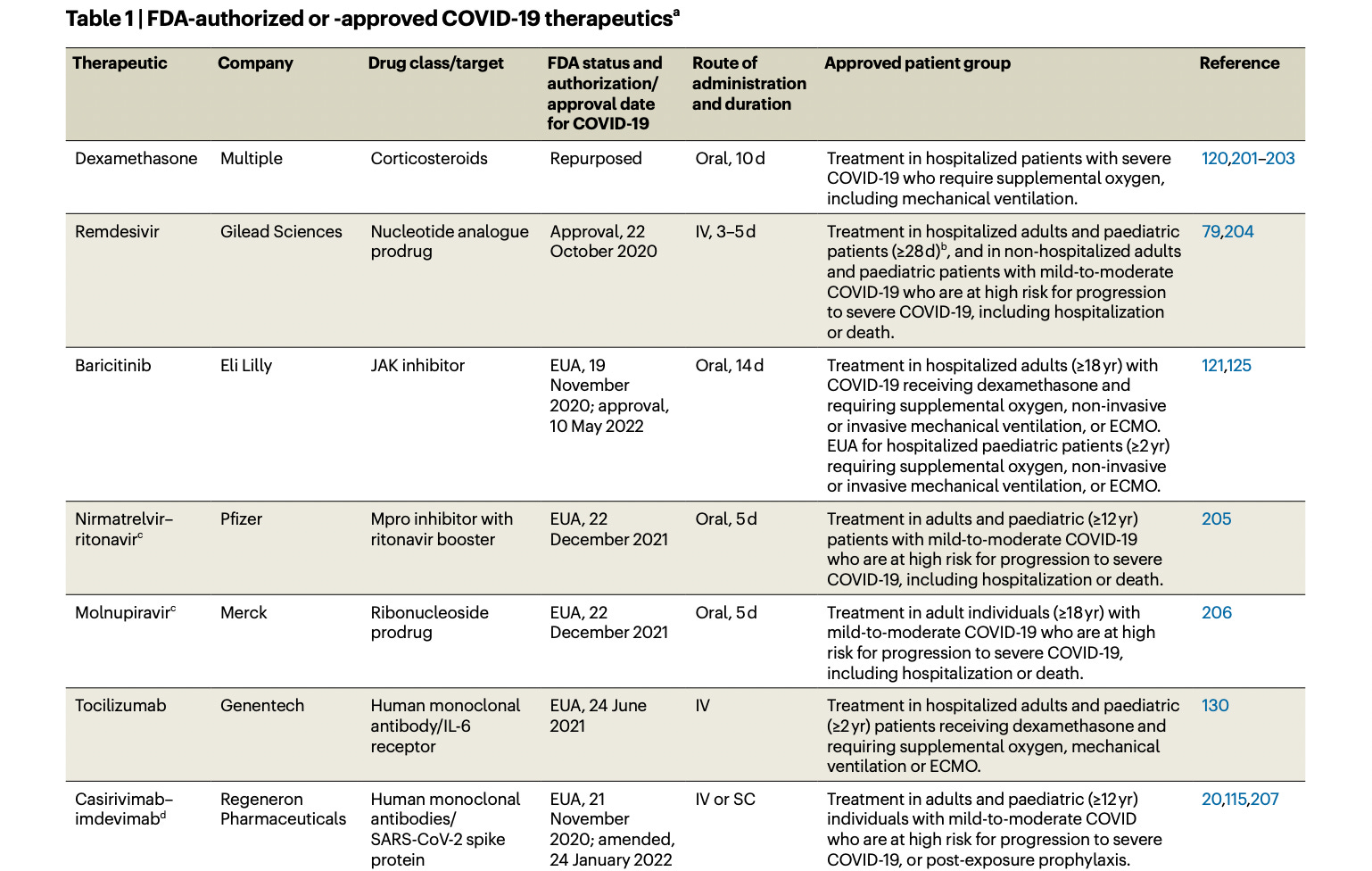
During the COVID19 pandemic, a small handful of drugs and therapeutics helped save lives. RECOVERY showed the value of dexamethasone in patients hospitalized and receiving O2, and those on the vent. Baricitinib also had positive randomized data, and Tocilizumab was validated by the RECOVERY group. Paxlovid only has positive data in unvaccinated high risk people who have not had COVID.
As of 2023, the landscape of drugs looks like this:

But here is the kicker:
NONE OF THESE DATA APPLY to 2023 and going forward. Not a single one of these trials has assessed the value of these medications in the current world where many people have had COVID multiple times, and received multiple boosters. Not a single one of these trials applies to current circulating strains.
These data don’t apply.
Paxlovid is particularly bad. The fact that the Biden administration pushes this drug on vaccinated people who already had COVID is a failure of evidence based medicine. I am worried that Ashish Jha and Bob Califf have exaggerated the evidence for this product and undermined their credibility. I will be watching their future consulting closely.
Frankly, continued use of all these products is an EBM failure. We need to repeat RCTs for these agents in 2023. COVID19 is different today than in 2020. It is more often a bystander today, and seldom causes severe lung damage. Do these drugs work as they once did?
Years ago, Palmer Green, Adam Cifu and I argued that evidence should come with an expiration date.
We used the example of aspirin in primary prevention, which once had positive data in a world of skinny people who smoked, but no longer works in a world of obesity and scant tobacco. The same drug might work differently as time advances— and evidence needs reappraisal— was our message.
Of course, this is not just possible, but probable for COVID19. The disease is different now. The presentation is different, and every ICU doctor and hospitalist knows that we are not living in the summer of 2020.
If we do not repeat these studies, we will merely enrich drug companies, and possibly harm people through the side effects of medications that do not offer countervailing benefits. We have no idea if any of these drugs work in 2023.
Paxlovid has especially poor data, and the consistent pressure from this administration to prescribe it will someday be reminiscent of Tamiflu.
It’s not difficult to generate evidence for drugs that earn billions. Time to re-up this evidence base.
I'm not worried about Ashish Jha's and Bob Califf's credibility. They can worry about their own credibility. I no longer look to them for guidance and trust.
Thank you for being a champion for EBM and patients, Vinay.
D. Prasad....regarding your concerns that Jha might have undermined his credibility.... There's nothing to be concerned about. He ABSOLUTELY destroyed is credibility. See? nothing at all to be worried about! LOL. (what a bunch ass-hat clowns!)