
Do not assume beneficial interventions apply to higher-baseline risk patients
The TRACK trial of low-dose rivaroxaban in patients with kidney disease teaches an important lesson in EBM

Trials of therapies for patients with advanced chronic kidney disease (CKD) teach important lessons in evidence based medicine. You don’t have to be a kidney specialist to learn from such trials.
JAMA has published the TRACK trial of low-dose (2.5 mg) rivaroxaban every 12 hours vs placebo in patients with advanced CKD and either established vascular disease or high-risk for vascular disease.

The thinking
The most common cause of death in patients with CKD is cardiovascular. Yet numerous trials of interventions which have shown benefit in standard cardiac populations have failed in CKD—re statins.
Low-dose rivaroxaban has been shown (in two trials) to modestly lower major adverse cardiac events (MACE) in patients with coronary artery disease (COMPASS) and patients with symptomatic peripheral artery disease (VOYAGER PAD). Why not try it in high-risk patients with CKD?
The trial
The TRACK trial screened nearly 6000 patients to include nearly 1500 who were randomized to receive low-dose rivaroxaban or placebo. Pause there and note the highly selective nature of the trial. (Good on the investigators for showing this important trial feature.)
Inclusion required the patients to have had dialysis-dependent kidney failure or CKD stage 4 or 5 not receiving kidney replacement therapy (estimated glomerular filtration rate ≤29 mL/min/1.73 m2). Patients also had to have actual coronary, peripheral or cerebrovascular disease or be at high-risk for it.
Exclusion criteria were even more extensive. Bleeding, indication for anticoagulation (AF), drugs that could interfere with rivaroxaban metabolism, liver disease, heart failure, anemia, kidney transplant and many more conditions were causes for exclusion.
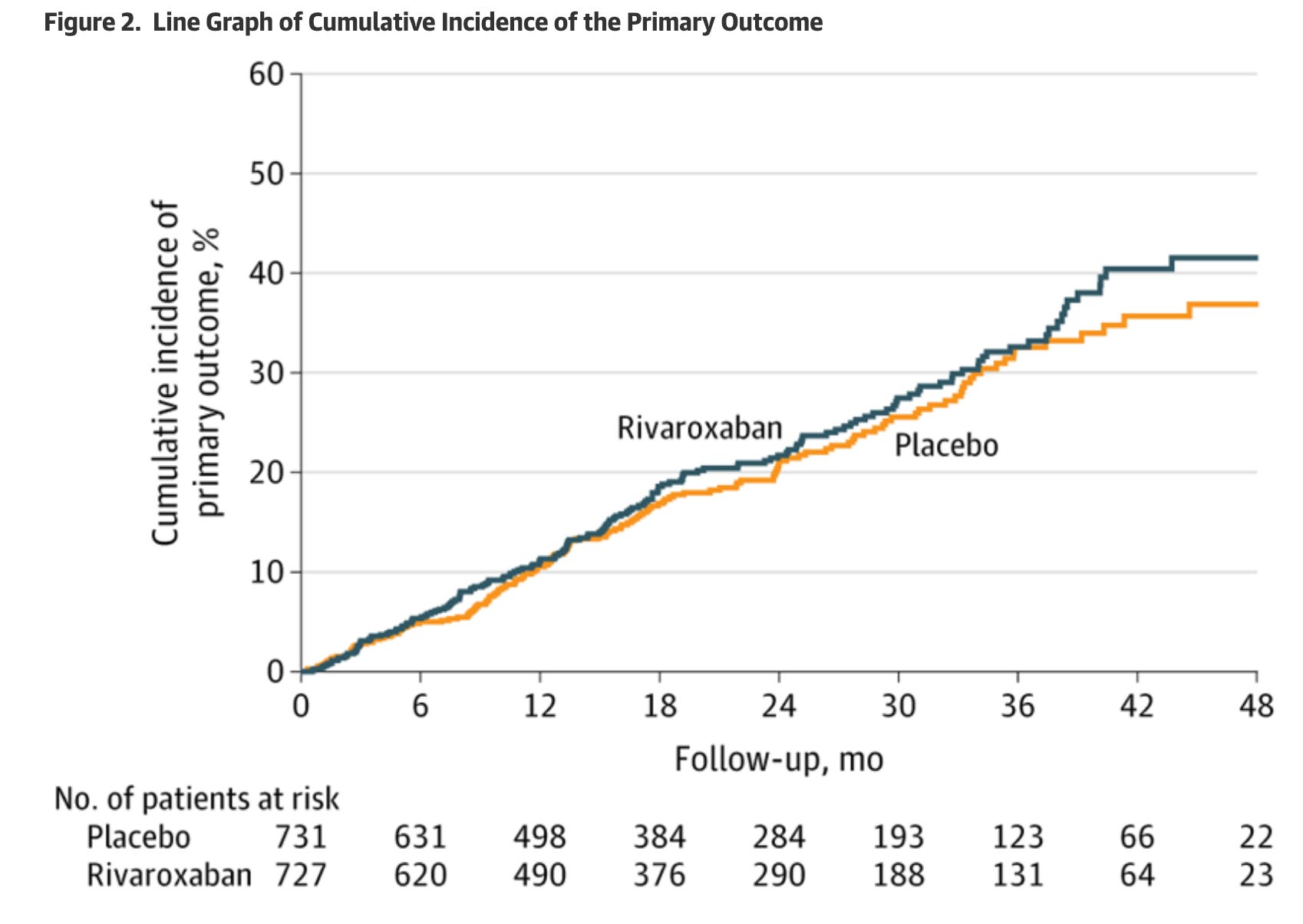
The primary outcome was a composite of CV death, MI, stroke or PAD event. The primary safety event was major bleeding.
The trial was powered to find a 25% reduction in the primary endpoint assuming an event rate of 10 per 100 patient-years in the placebo arm (which was quite reasonable).
Patients were 63 years old; 30% female and half were on dialysis.
Results
After a prespecified interim review of the data after only half the expected events had occurred, the data and safety monitoring board recommended early termination of the trial due to concerns over net harm and an extremely low probability of efficacy.
A primary outcome occurred in 164 patients (22.6%) in the low-dose rivaroxaban group and 151 (20.7%) in the placebo group (13.0 vs 11.8 events per 100 person-years; hazard ratio, 1.09 [95% CI, 0.87-1.36]; P = .46).
Rivaroxaban also showed no signal of benefit in any of the secondary outcomes. Nearly every outcome was numerically higher in the active arm.
Major bleeding was higher in the rivaroxaban arm (5.1 vs 3.4 events per 100 person-years; hazard ratio, 1.51 [95% CI, 1.02-2.22]; P = .04).
Comments
Whenever you have a nonsignificant trial, it’s always worth asking whether the signal is not there or did we not detect it. In other words, what are the chances of a false negative? That is one of the risks of early trial termination.
Here, with 95% confidence intervals having a lower bound of 0.87, I think it’s unlikely to have found a 25% reduction. What’s more, even if benefit was underestimated it would be countered by a 50% greater risk of major bleeding.
Clearly low-dose rivaroxaban should not be used in this patient population.
The teachable critical appraisal point is that high-risk does not guarantee greater benefit. The control arm event rates were highest in TRACK (12% per year) vs VOYAGER PAD (8% per year) and COMPASS (5% per year).
But low-dose rivaroxaban worked in COMPASS and VOYAGER PAD. In COMPASS, low-dose rivaroxaban plus aspirin vs aspirin alone, MACE reduction was 24%. In VOYAGER PAD (PAD patients), rivaroxaban + aspirin vs aspirin alone, MACE reduction was 15%.
CKD therapeutics teaches this high-risk-does-not-guarantee-benefit lesson well.
The authors and editorialists posit that non-thrombotic cardiovascular pathways may dominate in CKD patients; they also note the higher bleeding risk in CKD patients. I would argue the cause is less important than the observation that you cannot assume a therapy’s relative risk reduction applies to higher risk patients.
There are many other examples of interventions that work in the non-CKD populations but do not work in patients with CKD.
Statins are the classic example. More than 25 RCTs have shown statin benefit in primary and secondary prevention, but the 4D and AURORA trial both found no benefit for statins in patients with advanced CKD. The internal cardioverter defibrillator has shown benefit in patients with heart failure, but the ICD2 trial of the ICD in patients with CKD was stopped for futility.
Conclusion
Trials in patients with CKD are always worth your attention.
The first reason is that of course we want to find therapies to help this group of high-risk patients. And the only way to prove benefit is with the RCT.
The EBM reason to pay attention to CKD trials is the concept of treatment effect heterogeneity. Most therapies have a sweet spot of benefit.
In the case of low risk, it’s hard for a therapy to make low risk lower. Harm can outweigh benefit. See our upcoming post on GLP1a.
In the case of high risk patients, competing risks, disease heterogeneity, and higher adverse events (lower drug clearance or drug interactions) can lead to lack of benefit.
The extension of this concept is that we should be very cautious extending trial results to patients unlike those enrolled in trials.
A great post about a well done study. The take-home point that the results of RCTs apply to only those patients who are most like patients in the trial is the most important.
Thanks for writing up this study!
"competing risks of death"
First, let's just point out that remarkable fact that 24% of the patients died in this trial that had a median followup of 1.7 years (and only 20% still at risk/followed at 3.0 years).
There were 354 deaths out of the 1458 people in the study. Ranked causes:
1. Sudden cardiac death (149, 42%)
2. Infection (64, 18%)
3(t). Other CV causes (60, 17%)
3(t). Other non-CV causes (60, 17%)
4. Unknown (21, 6%)
Once you get past the (presumed) arrhythmias and infections, you really only have about 1/3 of the causes of death left. Narrow that to (non-sudden) CV deaths (MI, stroke, CHF), and it's maybe 1/6 of the population. It's almost like trying to demonstrate a benefit in reducing CV events in patients with lung cancer.