
Do you think a bone marrow transplant is worth it?
Doubt and pain

Years ago, I was late to a dinner party at a new, trendy downtown restaurant. I had been working as an attending on the bone marrow transplant service, and the day got away from me. I had to take care of a patient who had a serious adverse reaction when she received her stem cell infusion. Another patient was suffering from a catastrophic fungal infection, and graft versus host disease threatened the life of a third.
Meanwhile, there were 20 more patients to see on the transplant floor and 3 more in the intensive care unit. The dinner was supposed to begin at 8pm, but I didn’t arrive till 9pm. I sat down at the table: preoccupied, disheveled and flustered.
There are nights when you the leave the hospital, but your mind remains behind. You could be at dinner, with friends chatting volubly, or at home with loved ones, but your brain replays the day’s events, and wonders, one more time, if you are missing the real reason Ms. Jones is still having fevers. Then someone interrupts your thoughts.
“You are a space cadet— what are you thinking about?” my friend Thomas asked me.
“Sorry— my mind is still at work.”
“What were you doing exactly?” he asked— there were 5 people at dinner and none were in medicine.
“I am on bone marrow transplant— which basically means that for some people with blood cancer we transfer a different person’s immune system into them. We hope that the new immune system will recognize their cancer as a foreign invader, and eradicate it, but unfortunately, sometimes it doesn’t or sometimes it thinks the healthy body is foreign, and we always walk the tightrope of hoping it attacks the cancer more than the person.”
Some studies suggest that allogeneic stem cell transplant— the procedure itself— can kill as many as 1 in 5 patients.
“The people who get a transplant, they can get very sick?” Thomas asked.
“Yes, absolutely. And honestly— that is where my mind was— I’m sorry— sometimes, I keep thinking about if we might be missing something."
“Do you think it is worth it, these transplants— you only do it because you have to do it?” Thomas’ girlfriend Sarah asked— I didn’t know her well, and she struck me as generally shy and introverted, but she posed the question with interest.
“To be frank, I struggle with it.” I told her my general view. Yes, absolutely, all of us who have done bone marrow transplant have seen people that we were certain would die, but are now cured. At the same time, we have also seen many patients suffer greatly from the procedure, and no one who transplants should make the decision lightly.
“But what really bothers me about bone marrow transplant is that for many people undergoing it— we don’t know for sure…”. I continued, and I told her about some work we had been doing. (it would eventually be published years later).

In our paper, we examined the recommendations made by the transplanting society. Of course, they often favor transplant— that wasn’t surprising though.
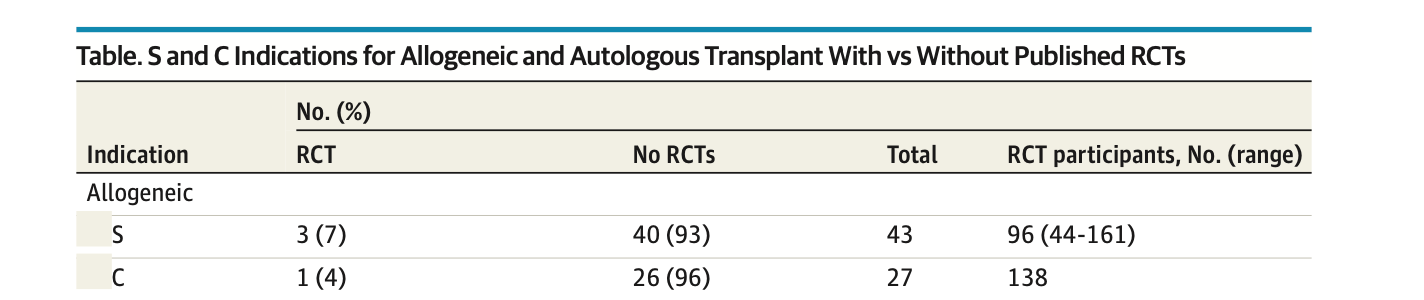
What was surprising was that we found that most S recommendations— meaning a standard of care recommendation (a strong recommendation)— weren’t supported by randomized data. Worse, the studies that did support transplant often left considerable doubt. We concluded that for many diseases— we have uncertainty— and randomization is not just possible, but necessary. Here is what we say:

As I spoke, I felt Sarah’s demeanor change. She listened intently to my explanation. She asked what I thought about the doctors who recommend the procedure, “Why are they so confident, if they have doubts?”
I told her my view— that every doctor who recommends a transplant does it because they truly think it is best. At the same time, the profession has— in my opinion— not been good about testing dogma. And finally, I told her my personal view, “I always struggle with doubt— it plagues me— and sometimes I am not sure if we should be doing it.”
She looked down into her drink, her eyes were wet.
“I don’t tell many people this,” she began, “my sister… she was 14 months older than me… she died after a stem cell transplant. And, like you, I have only ever struggled with doubt.”
A moment later, she excused herself to the restroom. Thomas told me that he had no idea. Over the next few weeks, I would reach out to, and eventually meet Sarah on several occasions to talk to her about her sister, apologizing profusely if I had put my foot in my mouth, and then, over time, answering questions she had had about her sister’s care. Questions that had lingered for more than a decade. Questions that still woke her from sleep. She was grateful to talk about it.
Uncertainty— doubt— every doctor has felt it; many of us push it down and suppress it. We try to carry on with confidence we wish we had, but none of us feel the pain of doubt— the sharp agony of not knowing if we made the right decision— the way a sister feels it. Two sisters— 14 months apart— and one lives only in the heart of the other. To me, it is the reason medicine— our profession— has an obligation to test what we do, to know with confidence that we are making the right decision.
Vinay
The last paragraph says it all, and this is one of your best! Thanks for being courageous and always questioning the group think.
Vinay,
Beautifully written. As an emergency room nurse, I see my share of failed procedures. It often makes me doubt how aggressively we treat patients today. But then my dad was diagnosed with primary myelofibrosis and relying on blood transfusions to stay alive for months. He got a bone marrow transplant. He said “I worked with the Red Cross in Afghanistan in the 90s and I would do that 1000 times over what I went through recovering from this procedure”. But he is strong and stubborn with a sense of purpose and pushed through. He is now 7 months out with perfect lab work and back to himself in almost every way. If we didn’t take these risks with these procedures, we wouldn’t have the survivors and the ones we lost would most likely still be lost. So in many ways, I think we should be doing these things. But as providers, if we didn’t deliberate about the ramifications, I think that would be worse.