
Drug-eluting coronary stents: a masterclass in (broken) evidence translation?
The genie isn't going back in the bottle, but I hope someone can explain the drug-eluting stent phenomenon to me. Because evidence doesn't seem to.

When I was at Indiana back in the 1990s, we called an ICD by a company’s brand name. At IU, all ICDs were “PCDs”. PCD was Medtronic’s brand name. I didn’t realize it at the time, but this was pro-level marketing.
A similar thing has happened with coronary stents—at least in my neighborhood. Now it is Xience, a brand of drug-eluting stent (DES) from Abbott.
The story today is how the drug-eluting stent crushed its competitor the lowly bare-metal stent (BMS)—despite costing 3x more and requiring longer duration of antiplatelet therapy. You’d think it was evidence. But read on.
This topic is in my head because we’ve been covering it over at Cardiology Trials substack.
The DES story begins in 2004 when the TAXUS-IV trial showed that a drug-eluting stent reduced angiographic restenosis vs a bare-metal stent.
Regular readers of Sensible Medicine, however, would likely know not to rejoice over the positive findings. Because the primary endpoint was a surrogate endpoint—as the condition of the vessel was merely a picture of a vessel, not an actual cardiac event. In fact, TAXUS-IV heralded future trials in finding no difference in hard outcomes such as CV death, MI or stent thrombosis between the two stent types.
The main focus of today’s post is the huge NORSTENT trial, published in 2016 in NEJM. More 9000 patients randomized to either a drug-eluting stent or bare-metal stent.
The primary endpoint was CV death or MI at 5 years. Just that. Hard endpoints. Repeat revascularization (another stent), stent thrombosis and quality of life were secondary endpoints. (A detailed review is over at Cardiology Trials.)

Before giving you the results, I should say that drug eluting stents underwent substantial technical iterations. NORSTENT however used contemporary second-generation stents.
Results:
At 6 years, 16.6% of patients in the DES arm vs 17.1% in the BMS group had a primary endpoint. The HR was 0.98 95% CI 0.88-1.09 and P-value of 0.66.
Here is the KM curve:
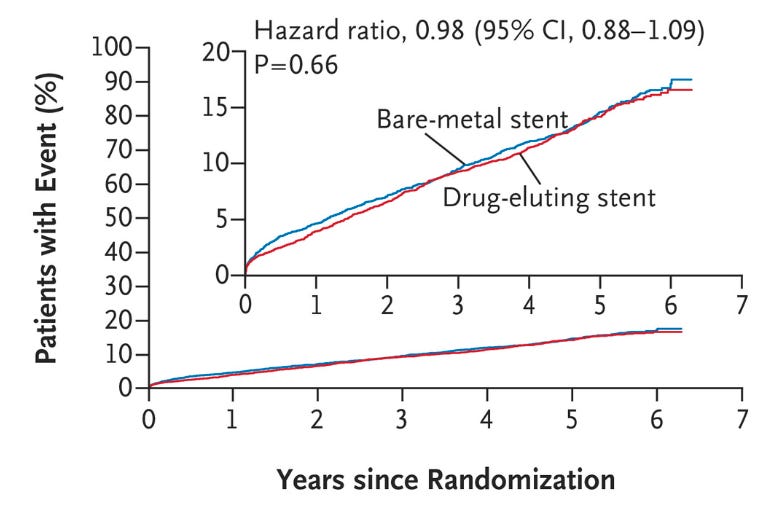
That is about as negative as negative can be. These were 63 year-old patients who had severe CAD, about a quarter were having an MI, 40% had multi-vessel disease and 50% had some complexity of the lesion. IOW: a representative sample.
Coronary revascularization (the placement of another stent was 3.3% higher (absolute risk increase) in the BMS arm, driven by a doubling of the rate of target lesion revascularization (5% vs 10%) in the BMS arm. Stent thrombosis, which is a terrible outcome, almost always leading to MI or death, were slightly lower in the DES arm (0.8 vs 1.2%).
But. But. The composite of CV death and MI capture the outcomes we care about after coronary stenting. If stent thrombosis or repeat revascularization were huge factors, it would be seen in a difference in MI or CV death. It was not.
Quality of life measures were not different. So the slightly higher rate of repeat procedures in the BMS group did not effect how people felt.
These results were not different from a smaller trial, called EXAMINATION. In this trial of 1500 patients, a primary endpoint of all-cause death, MI, and any revascularization at 1 year did not significantly differ at one-year.
My Questions
A brief search revealed that drug-eluting stents cost many times more than a bare-metal stent.
In multiple trials, including one of the strongest RCTs in cardiology, NORSTENT, there were no differences in major clinical outcomes.
Yet, DES have become so established that it would be silly to even ask an interventional cardiologist to use a bare-metal stent.
This is not an esoteric academic question. Millions of cardiac stents are placed each year. Coronary stenting is one of the most common procedures not just in cardiology but in Medicine.
I raise this issue not because I aim to bring back bare-metal stents. That ship has sailed. I raise it because it is one of best examples of how something gets established despite little evidence of benefit.
Since I am not an interventional cardiologist, I cannot tell you how it happened. I suspect factors included: marketing, marketing, and a decoupling of cost and value.
People-in-the-know should feel free to explain this to me in the comments. We would also welcome an explainer from an interventional cardiologist.
Greatly appreciate and enjoy your articles. On this rare occasion we might have to disagree. UK interventional cardiologist here with some historical perspective. Benefits of drug eluting stents (DES) were never about reducing incidence of death or non-fatal heart attacks, the primary endpoint of NORSTENT. Prior to DES, the Achilles heel of PCI was instent restenosis (ISR) to the extent that PCI would be avoided in those patients with lesions most likely to restenose, typically diabetics with small vessels needing long stents. ISR was a huge issue in the era of bare metal stents (BMS) with masses of research into treatments- remember the use of brachytherapy? DES revolutionised practice and patients who would not have been offered PCI previously are now treated routinely with good outcomes.
The patients included in NORSTENT are probably not typical of those treated today- the data provided is limited but there seem to have been more patients than we see today in whom restenosis rates would be predicted to be low- focal disease in fairly large vessels and remarkably few diabetics.
I would suggest that NORSTENT was not primarily designed as a restenosis/revascularisation trial but even so there was a significant difference in revascularisation rates favouring DES. Should we be surprised the difference was not greater? I suggest not- many factors influence the decision to offer repeat coronary angiography, a necessary prelude before repeat PCI. In general repeat revascularisation is for treatment of angina (much less often for heart attack/unstable angina), and as you argue so elegantly in previous articles, PCI does not confer any prognostic benefit (ie reduction in death or heart attack) over optimal medical therapy and risk factor control in chronic stable angina.
Not all cardiologists went to universal immediate adoption of DES when they were introduced. For many years there was concern about the risk of late stent thrombosis compared to BMS, so that DES were sometimes avoided in patients at high bleeding risk who might not tolerate prolonged anti platelet therapy especially for those less likely to develop ISR. However the costs of DES have reduced remarkably since introduction and for whatever reasons, the risks of late stent thrombosis appear to have been over-stated (at least in contemporary practice), hence the universal adoption of DES.
Having come up just before the liberation of opioids for chronic non cancer pain and feeling like a lone voice screaming foul regarding addiction potential, I feel your pain here. As a former employee of a large hospital system that worshipped the Medtronic god, I feel your pain there! The companies learned a lot from the Purdue debacle with opioids; they learned how to be MORE savvy…the higher “up” I got in healthcare, the more “bought” arms of medicine there seemed to be. How does one stay healthy with a system like that??