


Exercise is Great but It’s Not a Cancer Drug
The CHALLENGE trial ignited social media with its great story of exercise as a cancer therapeutic. But liking a conclusion is not a reason to stop thinking.

The CHALLENGE trial tested cancer outcomes from a structured exercise program. NEJM published the study, more than a 100 news sites covered it, and hundreds reposted it on social media.
So you know the results were positive. Hugely positive, in fact. And who, I ask, does not love the story that exercise vanquishes cancer?

Sensible Medicine is a place to get the real story. This is a classic case when you have to let go of your love of great stories to see the details.
The Trial:
The stimulus to study structured exercise comes from observational studies that report associations between exercise and better cancer outcomes as well as preclinical studies that have (weakly) suggested that exercise may reduce the growth of cancer, possibly via metabolic or immune mechanisms.
CHALLENGE authors decided to test the effects of a structured exercise program in patients with colon cancer who had completed adjuvant chemotherapy. Eligibility for the trial required not dying from colon cancer, completing chemotherapy and having a functional capacity good enough to complete exercise tests.
Slightly more than 900 patients were then randomized to either general health recommendations or the structured program, which was intense. It included 17 “evidence-based techniques” for behavior change, including frequent mandatory in-person behavioral-support sessions and supervised exercise sessions. Emphasis on mandatory and in-person.
During the second 6 months, patients had more of the same but could have some sessions via phone. During the last 2 years, patients attended 24 mandatory monthly in-person or remote behavioral-support sessions combined with a supervised exercise session. The supplement took 50 pages to describe the many details of the structured exercise program.
The primary endpoint was disease-free survival, which sounds simple but was actually composite of many things: freedom from recurrent colon cancer, new primary colon cancer, a second primary cancer or death from any cause.
The results were amazing.
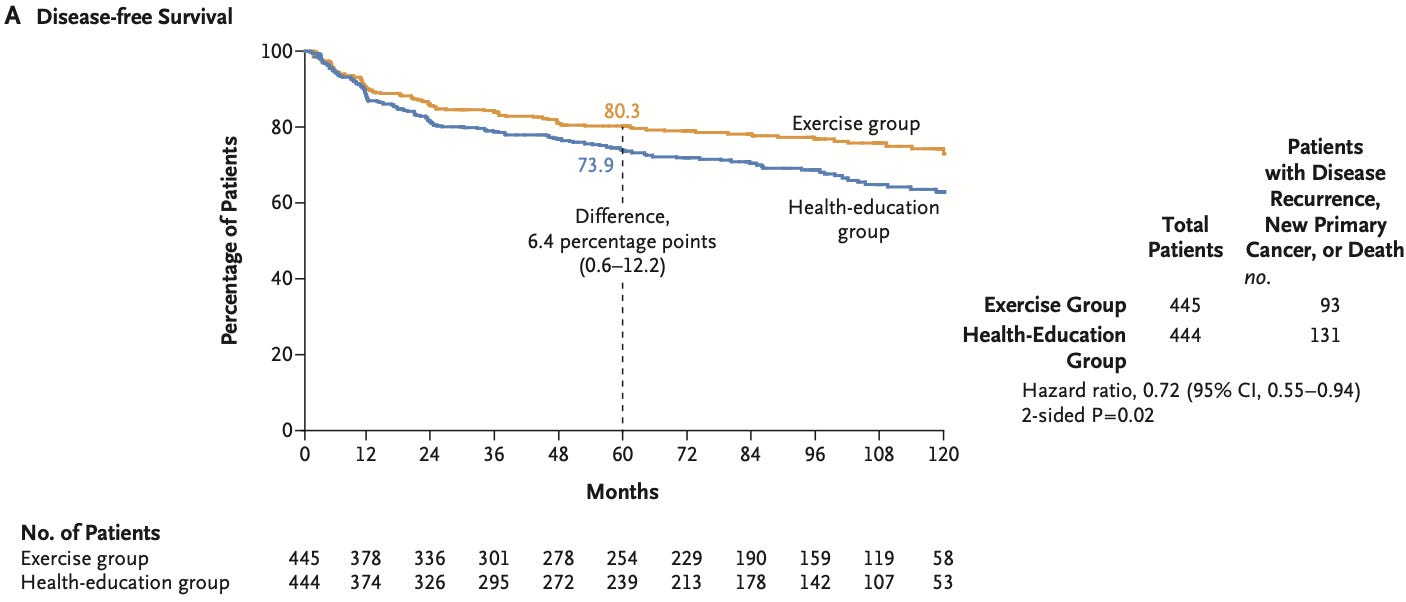
At a median follow-up of nearly 8 years, the primary outcome of disease-free survival occurred in 21% of those in the exercise group vs 29.5% of those in the health education group. The relative risk reduction was 28% with a hazard ratio of 0.72 and 95% confidence intervals of 0.55-0.94 and a p-value of 0.02.
The 5-year disease-free survival was 80.3% in the exercise group and 73.9% in the health-education group (difference, 6.4 percentage points; 95% CI, 0.6 to 12.2).
Drivers of the primary endpoint included both recurrent cancer and overall survival.
In fact, the relative risk reduction for overall death of 37% (HR 0.63; 95% CI, 0.43 to 0.94) was even larger than the risk reduction in the composite endpoint.
Remarkable was that exercise also seemed to reduce recurrent colon cancer (65 vs 81 patients) as well as new primary cancers (23 vs 42 patients).
The authors concluded that this 3-year structured exercise program “resulted in significantly longer disease-free survival and “findings consistent with longer overall survival.”
Comments and Appraisal
The first thing to say is that I love exercise—in my personal life and as a cardiologist. I also appreciate the authors’ attempt to study exercise in rigorous RCT fashion.
While I want this story to be true, there are at least seven reasons to be cautious. These are mostly internal validity concerns. But there are also major external validity issues as well.
First, before looking at the methods, the 37% reduction in all-cause mortality is implausible and rivals many proven cancer therapies. For example, this is similar to the mortality reduction with Trastuzumab (Herceptin) in HER2+ breast cancer—a revolutionary finding.
Second, if you posit exercise provides a massive mortality benefit, there should be some effects of exercise. CHALLENGE reported almost no between-group differences in typical exercise parameters. There was zero differences in body weight, waist circumference and a mere 30 meters longer distance in the 6-minute walk test.
Third, the Kaplan-Meier survival curves for disease-free survival begin separating at 12 months while the death curves take 4 years to separate. I am not a cancer doctor, but a tiny difference in exercise dose (as evidenced by the lack of objective measures) is not enough to reduce cancer recurrences that rapidly. This finding suggests suboptimal randomization, which is not surprising given the fact the ambitious complicated trial took 15 years to enroll.
Fourth, poor adherence to the exercise regimen further reduces plausibility. Nearly half of the patients in the exercise program did not complete the treadmill protocol at three years and a third did not complete the 6-minute walk test. These patients were included in the intention-to-treat findings—and would have the effect of reducing between-group differences in exercise.
Fifth, the authors originally designed the trial to detect differences at 3 years. This required 380 events to have sufficient statistical power. Due to slow recruitment and a slower-than-expected event rate they changed to a five-year analysis. Yet they still had far less than the expected primary endpoint events (224 vs 380). This reduces statistical power and raises the possibility of false positive findings—which is consistent with the biological implausibility. What’s more, the KM curves show most of their separation after 3 years. A stronger paper would have included the pre-specified 3-year results, which may have been non-significant.
Sixth, while the first five concerns relate to the conduct and the design of the trial, there is also the inherent challenge of strategy trials: different attention in the two groups. In CHALLENGE, the structured exercise group received an incredible amount of intervention in both behavioral modification and exercise. This makes performance bias highly likely, as evidenced by the large differences in the quality of life questionnaires.
Seventh, there are serious challenges in external validity or generalizability of the CHALLENGE trial. The difficulty in enrolling patients (it took 15 years) speaks to the complexity and intensity of the behavioral and exercise program. The authors don’t tell us how many were screened to enroll these 900 patients. I suspect it was a lot. What’s more, enrolled patients were young (age 61) non-obese and performed well on baseline measures of function. Even if you accepted the results as presented it would apply to a fraction of patients with colon cancer.
The cost and healthcare system implications of accepting this protocol would be massive. In the same way that regulatory trials for drugs or devices require multiple positive trials, we should feel the same about CHALLENGE.
It was a great effort. The story is delightful. But liking the conclusion is not a reason to stop thinking.
SInce this trial had such a great response on social and regular media, I will keep this column open to all. No paywall. Yet please consider supporting Sensible Medicine for its role in non-industry-conflicted critical appraisal of medical evidence. JMM
You have some thoughtful critiques here. Regarding the points you raise:
1. Implausibility. This statement is made without looking at available data. There is observational data on exercise after cancer which has relatively large effects on survival. There are also very few randomised trials of exercise with long follow up, so we don't really know.
2. Lack of objective exercise effects. There were some differences in VO2max for example, arguably the most important measure.
3. 'Early' separation in survival curves at 12 months. This is an arbitrary distinction and not a strong criticism. Colorectal cancer tends to relapse quite early at around 15 - 18 months. If exercise is going to have an effect then 'early' separation like this is to be expected.
4. Poor adherence. I think that the adherence was quite good for an exercise study in inactive 60 year olds. Not sure what the argument is here - because adherence was poor, then the effect is smaller than it appears?
5. This is valid, but lower than expected event rate is endemic in oncology trials. The fact that the OS separation is more obvious after 3 years reflects the survival kinetics of colon cancer.
6. I'm struggling to think how more contact with the study team and physical therapists would prevent cancer recurrence. Consider that on the one hand, you are saying it is implausible that exercise has such a large effect, while on the other hand trying to claim that increased attention has a large effect.
7. Some misapprehensions here. I don't think anyone believes that the specific exercise intervention in this study is what made the difference, aside from the fact they tried quite hard. Given everything we know about exercise already, a reasonable takeaway is "exercise makes a difference, do more than you are doing now" if you are receiving curative intent cancer therapy. The patients were younger than the median age of diagnosis of colon cancer, but the benefits of exercise if anything increase in older patients. It is wrong to suggest this doesn't have broad applicability.
I dispute that the cost of accepting this protocol would be 'massive'. No clinical trial protocol is implemented verbatim in the real world. Again, it is not the specific protocol that matters. A real world implementation would largely be getting people to exercise to the already recommended level, which doesn't seem overly onerous or expensive. I have little doubt that such an intervention would be cost effective. Cancer therapy gets more and more expensive, and people are also getting diagnosed at younger ages, so the marginal cost of each recurrence only increases over time. Additionally, exercise prevents other diseases which further improves the cost benefit analysis. And in any case, even if no attempt is made to implement formal exercise programs, on an individual level it is important that a patient knows they can do more to reduce their risk of recurrence.
What does concern me about this study is the potential for informative censoring - ie. people who dropped out of the exercise arm were also more likely to have a recurrence due to being generally less well or more frail. I still think that is quite unlikely to eliminate the observed benefits of exercise, however. Timothée Olivier looks at this on X (https://x.com/Timothee_MD/status/1929411436272382303), and the curves still separate.
Been a physical education teacher and track coach for 45+ years a runner for 55+ years competitive, plenty of skin cancers been cut off my skin . We have exercised our whole lives . Way too many I have run with are dead from cancers . So I have my doubts about this study . But I sure feel better running and lifting and just trying to stay in shape at 70.