
FAME-2: One of cardiology's most influential trials, and, one of its most flawed
Few trials illustrate the need for blinding more than FAME-2. You won't believe what I will show you today.

When cardiologists see a narrowing in a coronary artery, the old way of measuring it was to eyeball it. That lesion looks like 40%. The problem is that another doctor might call it 70%.
Well, more than a decade ago, engineers designed a catheter that could measure the actual flow obstruction. Fractional flow reserve or FFR was born. Here is a picture:
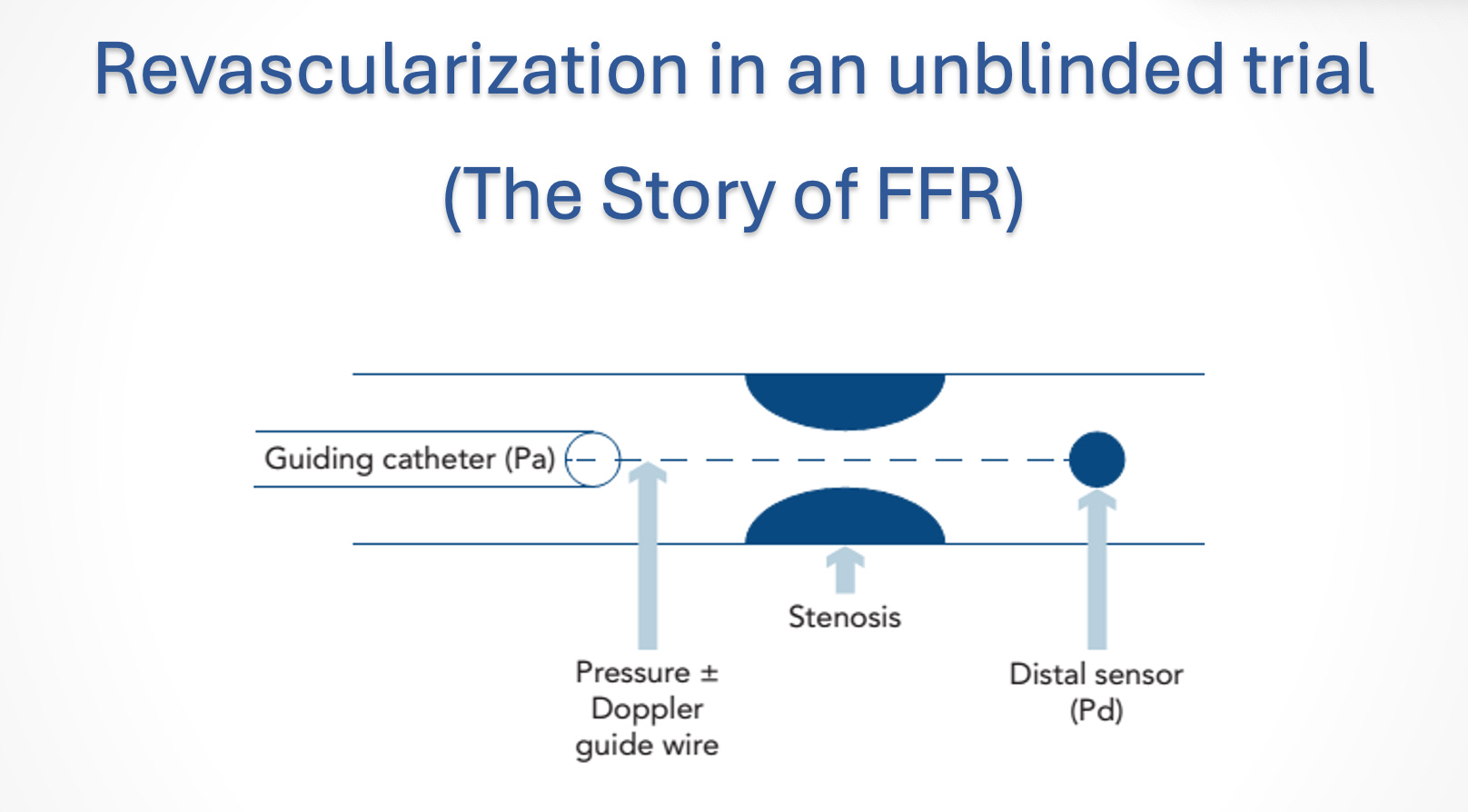
An FFR of 100% indicates no obstruction. By convention, cardiologists call an FFR ≤ 0.80 a “significant” flow obstruction.
Yet you won’t believe the seminal trial, called FAME-2, published in 2012. The question of the trial was how to best approach a chronic lesion in a coronary artery.
The background is crucial. Before FAME-2, previous trials had shown that stenting any chronic lesion would offer no benefits over medical therapy alone. People did not believe this because blockages are bad and must be fixed. Also, previous trials used the eyeball technique for measuring obstructions.
FFR would allow better identification of the really important lesions, thus improving outcomes over medical therapy with a stent. It could also reduce stenting by eliminating lesions that looked bad but had decent flow (> 0.80 FFR).
The trial protocol
Patients who had at least one flow-limiting lesion (FFR ≤ 0.80) on coronary angiography were randomized into two groups: FFR-guided PCI or medical therapy.
Pause there, because this is the key problem: one group got fixed; one group got tablets. Patients knew their assignment.
The choice of primary endpoint was also important; it was a composite of death, MI or urgent revascularization. These are typical endpoints.
The Results
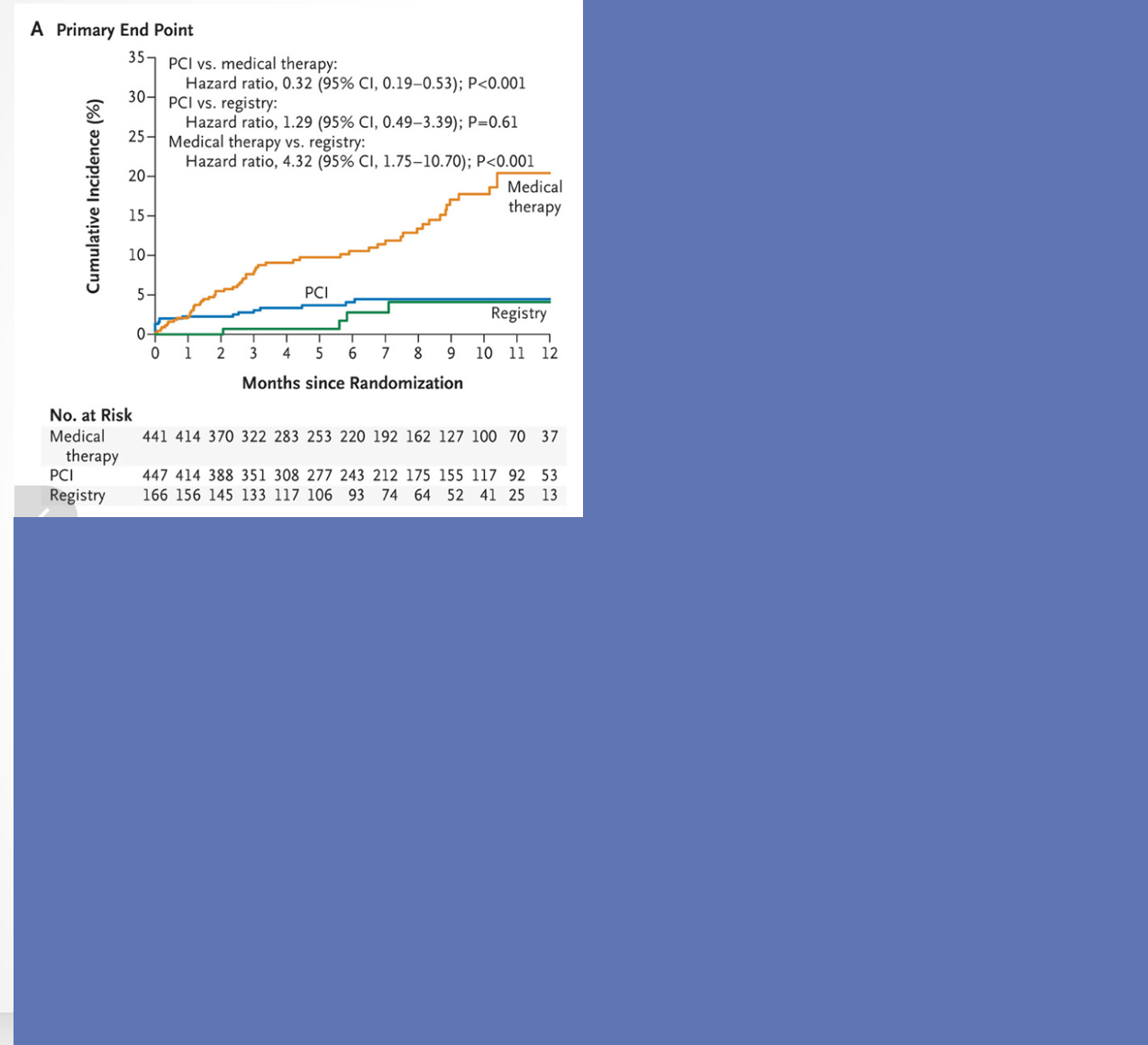
The above graph showed the massive dominance of FFR-directed stenting over medical therapy. The KM curves diverge after a month and continue to seperate. In fact, the authors were so concerned that they stopped the trial early as it would have been unethical (in their mind) to keep randomizing patients to medical therapy.
But. But. What about the components of the primary endpoint? I removed the boxes in the next image.
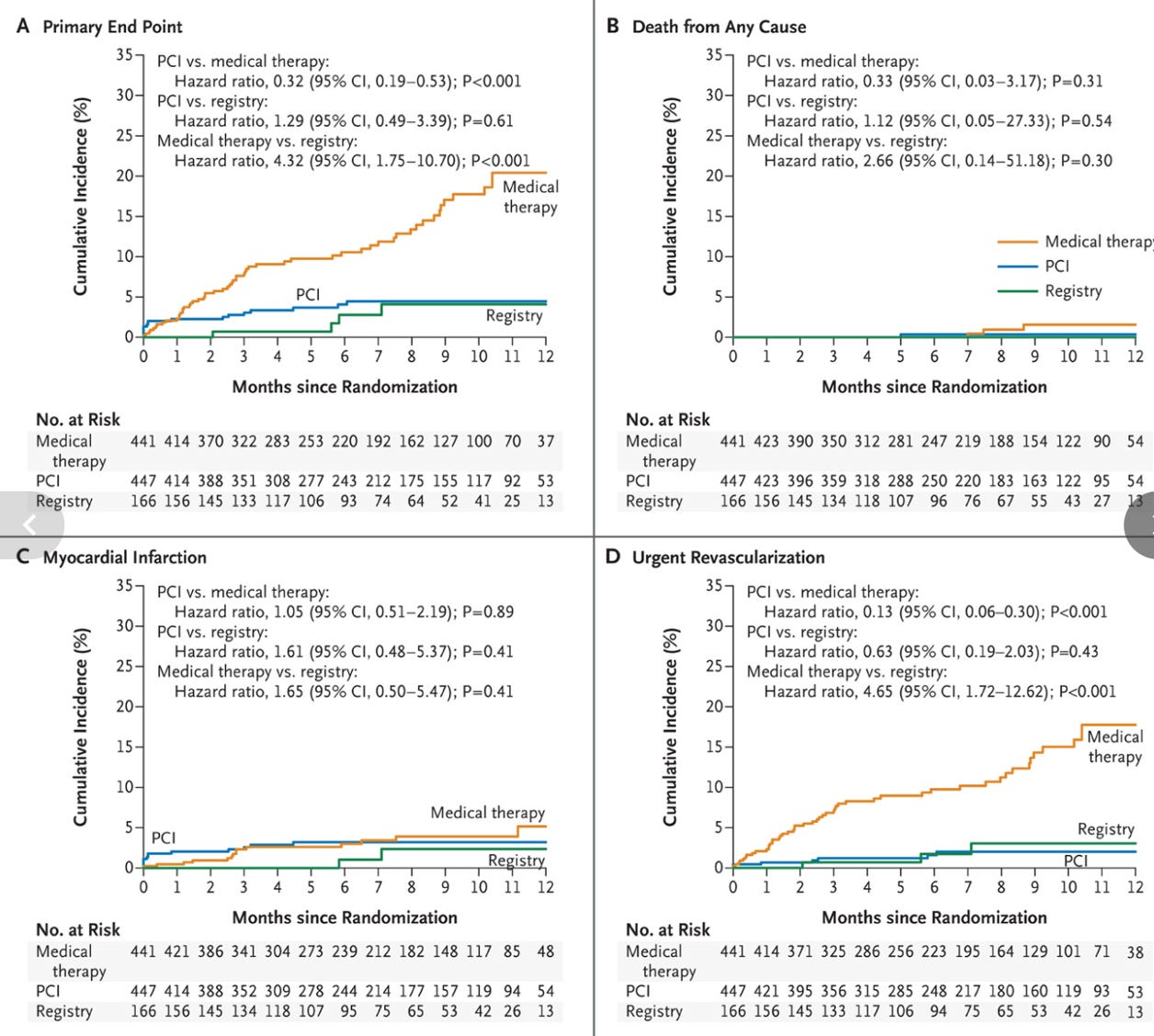
You can see that death and MI were not significantly different. All of the benefits came from urgent revascularization in the medical (stent subtracted) arm.
To be sure, avoiding an urgent revascularization is a positive because it is a buzzkill to have to have another procedure for symptoms of say chest pain or another MI.
The problem in FAME-2 was that patients knew that to get into the trial they needed to have a bad coronary lesion. Then one gets fixed and feels fixed, and the other group gets meds and feels unfixed.
A doctor named Christopher A. Rajkumar and colleagues from Imperial College London were interested in why patients had urgent revascularization in this trial. They took advantage of the fact that FAME-2 authors told readers the three reasons why patients had urgent revascularization.
These included worrisome ECG changes, elevated cardiac enzymes (suggestive of MI) or just symptoms. The first two were objective, the second was subjective.
This is best shown with pictures:
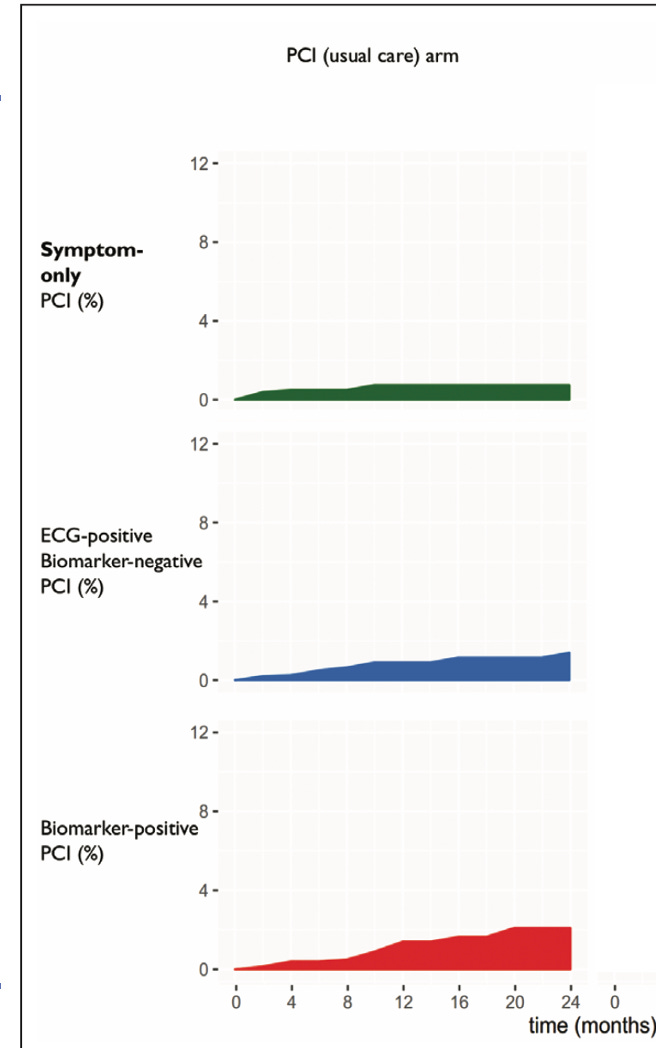
In the PCI arm, pts had an urgent revascularization in equal parts symptoms, ECG changes or enzymes. But look what happens in those told they were not stented:
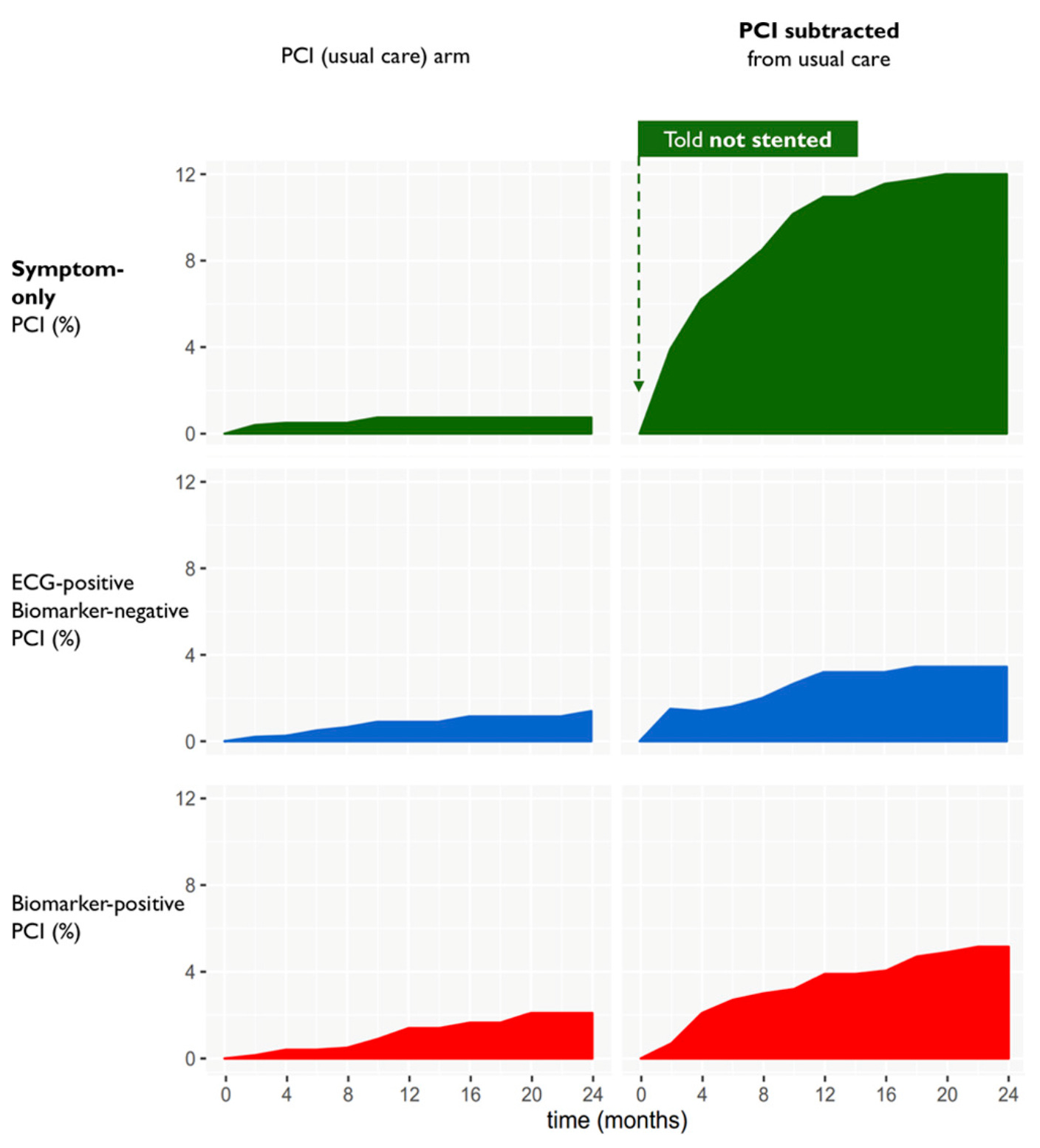
Symptoms rather than objective findings drove the positive endpoint. And almost all of the effect was within months. Why would that be?
Rajkumar and colleagues coined this effect faith healing and subtraction anxiety, wherein patients known to have a severe lesion were not fixed.
The next time they had even a twinge of discomfort, they sought care and the doctors fixed the lesion—with urgent revascularization. There were other papers discussed in their wonderful open access editorial.
I thought of FAME-2 because investigators recently published their 10-year results, which also show that positive effects were mainly driven by urgent revascularization.
You might think that given this flawed trial, that FFR would have been retired.
Well, you’d be wrong. FFR became a popular measurement, done even today, though there are iterations of it that proponents say are better.
But the whole thing rests on an utterly flawed trial. Flawed because of lack of blinding and a choice of an endpoint sensitive to unblinding.
I know; it’s a head shaker. But that’s how it goes.
My only solution to those who shake their head in amazement is to follow and support Sensible Medicine—as it is our goal to expose these problems and in so doing improve critical appraisal of medical evidence
If hospital systems had to pay out a DOLLAR for every stenting or angioplasty, they’d be orphan procedures. Rather than being the golden goose for CFOs and cardiology groups. Ditto joint replacement in 90 year olds, and 6-12 months of neoadjuvant chemotherapy in breast cancer, with marginal benefit over shorter course adjuvant therapy. In 78 year olds.
I believe that stenting and plasty are valuable and effective. In some. I also know that my utterly unexpected MI, with two subsequent stents and a total of 3 days’ admission w/o ICU, nor other complications was billed out at $284,000 (not a mistype) by the for-profit where I was treated. Would have been similar at the ‘nonprofit’ facility in the next town. Glad I had it. Appalled at the cost (forget the ‘but they don’t get paid that’ yada, yada: they were paid a LOT).
Put on an antiplatelet agent costing 10x the similarly effective older generic alternative. Because’reasons’. And because the cardiologist practice gets lunch every day, courtesy of XYZ Pharmaceuticals.
Go to any medium-to-large town in America, and look for the most impressive buildings in town. They will be:
State or county main offices
Insurance building
Hospital (cardiac wing, Ortho center, cancer center, women’s health annex…)
All built with your money. None of which are subject to competitive market pricing. All dependent on mandated/subsidized programs.
I most recently spent time in a metro of 125,000 or so. Two hospital systems that each cover a few blocks. Literally right next to each other. Competitive?
You bet. Competitive PRICING? Don’t be silly.
I’m no grizzled survivalist living in a trailer in the woods, hoarding cans of beans and ammunition. But, boy…sometimes I wonder.
I’m increasingly ashamed of my profession.
Very helpful analysis. I am not sure I agree with the premise that "avoiding an urgent revascularization is a positive..." The premise of the trial rests on the idea that an "urgent" percutaneous coronary intervention (PCI) is dramatically different that an "elective" PCI. In the first place, as you show, most of the "urgent" PCIs in the medical therapy arm were driven by subjective symptoms rather than any objective evidence of clinical harm. In the FAME-2 trial, then, the authors are proposing that doing elective PCI in 100% of patients with FFR<0.80 is clinical valuable because it prevents doing "urgent" PCI in 15% of them otherwise (the difference in "urgent" PCI between intervention [10%] and medical therapy [25%] arms. If one ignores the distinction between "elective" and "urgent" PCI, the proposition is absurd.
The fallacy here I believe is classifying a medical intervention as a "therapy" in one arm and an "adverse event" in the other arm. This methodology plainly stacks the deck in favor of the intervention. They made the same error in the EARLY AS trial.
Can you image if EPs did a trial of catheter ablation for asymptomatic AF and randomized half to ablation and half to medical therapy and then considered ablation for symptomatic AF in follow-up to be an endpoint? Of course catheter ablation would "win." I think we would all recognize this thinking as fallacious.