
Finally a Positive Trial for the Impella Ventricular Support Device
Some Lessons of the DanGer-Shock Trial

Let me craft a story about one of the worst-case scenarios in cardiology. A common cause of cardiogenic shock occurs when a blocked coronary artery (myocardial infarction or MI) causes the heart to fail. That happens because the obstruction to flow involves a lot of downstream heart muscle.
It’s a terrible scenario because if the doctor could only get that artery open fast enough the patient would likely survive. Cardiogenic shock from MI has a death rate of about 50%.
The problem is keeping the patient alive long enough to open the artery and then supporting the injured heart muscle until it recovers.
Interventional cardiologists have turned to support devices. First was something called the intra-aortic balloon pump or IABP. This device sits in the aorta and suctions blood out of the heart during systole and pumps blood into the coronary arteries during diastole. It makes a lot of noise but trials showed it ineffective.
Then came something called the microaxial flow pump, called Impella. It’s an ingenious device that goes across the aortic valve into the LV. It spins and spins and pumps blood from the failing LV into the aorta. It can deliver many liters of cardiac output.
The idea for Impella for cardiogenic shock is to support the heart’s output while the doctor opens the artery and then continue support for some days while the injured heart muscle recovers.
So far I’ve told a nice story. But.
Nice stories are rare in medicine. It turns out that a) Impella can cause problems, such as bleeding or limb ischemia; b) some patients are too far gone to save; and c) many patients would survive without the Impella.
And there’s more negatives: three small trials of Impella (and a meta-analysis of these three trials) all showed that the Impella did not improve survival in cardiogenic shock.
Thing is that doctors have been using Impella for years. Many tens of thousands of these devices have been implanted—at great cost—in the absence of trial-level support.
American doctors say they know Impella works. “We have patients who would not have survived their MI without it,” goes the common saying.
This is why the DanGer-Shock trial had to be done in Denmark, a place where doctors are perhaps a little less sure of themselves.
The Trial
Dr. Jacob Mollør, and colleagues at Odense University, in Denmark worked for 11 years to randomize 360 patients—with just the right amount of cardiogenic shock due to acute MI—to either have the pump or have regular PCI and heart care.
Seriously, it took 11 years to select these patients. The trial was first planned for Denmark alone, but then Mollør had to expand to Germany. I will come back to the selection process.
The results supported the the contention of many cardiologists.
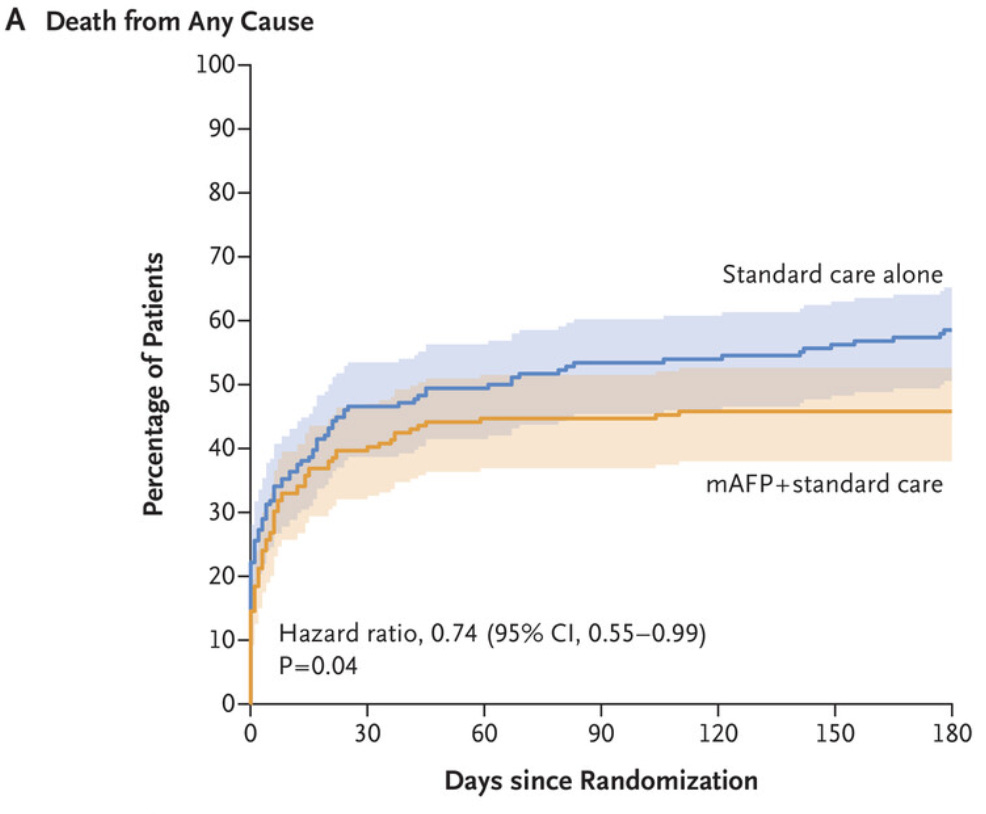
At 6 months, death from any cause (the primary endpoint) occurred in 45.8% of patients in the Impella arm and 58.5% of those in the standard care arm. That 12.7% absolute risk reduction calculates to a relative risk reduction of 26%. Hazard ratio 0.74 (95% CI 0.55-0.99). The p-value makes it at 0.04.
Safety events were higher in the Impella arm. The overall composite safety endpoint occurred in 24% of patients in the Impella arm vs 6% in the standard care arm. And the harms were serious, including a twofold higher rate of serious bleeding and dialysis, a fivefold higher rate of limb ischemia and a nearly threefold higher rate of sepsis with a positive blood culture.
The key thing to remember about these safety events were that many if not most would be included in the primary endpoint of death. IOW, if higher rates of bleeding or dialysis were so bad, it should have negated the lower death rate in the main results. It did not.
Putting it together and Mention of Another Study
I wrote about this trial over at TheHeart.org site. There’s more details there.
DanGer-Shock is a positive trial. But there are caveats. The main one being how hard the investigators had to work to find patients that stood a chance of benefiting. Eleven years of looking.
They used markers such as low blood pressure, lactate levels (a marker of low perfusion to the body) and the need for vasopressors to support the blood pressure. But if patients came to hospital with poor brain function or right ventricular failure, they were excluded.
The job of doctors now is to use wisdom in selecting these patients most likely to benefit. We need to choose patients just like those in DanGer-Shock.
In the matter of choosing the right patient for this device, there are other forces to consider. Doctors and hospitals are rewarded financially for using this device. And the device is costly.
Yes. Sadly. There are dualities of interest.
I point you to a recent study that explored payments to doctors from the Impella maker and subsequent use of the device.

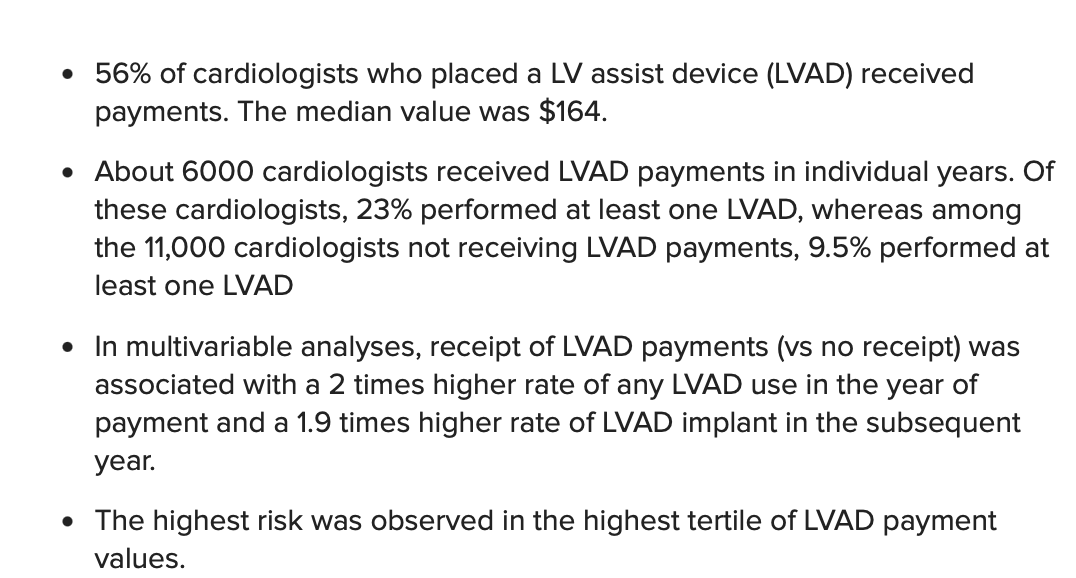
I covered this on my This Week In Cardiology podcast. TheHeart.org | Medscape Cardiology also publishes the transcript of the podcast. Here were the main findings of the JAMA study: (LVAD = left ventricular assist device or Impella):
Conclusions
The first is a scary one. Impella has been used for a decade or more. DanGer-Shock has been the first positive trial. Other trials have been negative.
What if the DanGer-Shock trial was negative? Imagine the harm that our profession would have done.
My grand idea is that we should be doing DanGer-Shock-like trials before widespread acceptance of new devices. If regulators reimbursed doctors only if use of the device was part of a trial, DanGer-Shock could have been done in 11 months, not 11 years. Then we would know a) it works and b) for whom.
We should require proof (or at least a strong signal) of benefit before a costly invasive treatment is accepted. We do it for drugs, we ought to do it for devices.
My second conclusion is to underscore the tension between profit-driven healthcare companies and the care of patients.
Payments to doctors and subsequent increased use of that product is unseemly.
But at least in this case we have one trial showing benefit for one indication for this device. If you have cardiogenic shock, and your life is saved by use of this device, you will be happy for the profit-driven innovation.
Let’s see what DanGer-Shock does to sales of the device. Since it took 11 years to find 360 patients, my thesis is that we should not see an increase in usage.
And it’s only one trial, so it’s still possible that the perceived advantage was a matter of random chance.
The trouble with this, and with drugs, is that the doctors prescribing the intervention in the real world stray from the patient selection criteria (and hence what was proven) in the research, so the intervention ends up being used more than it ought to be, with even less benefit (and more harms). If you use it in somebody who didn’t need it (because they would have recovered anyway) and they get better (as they would have done regardless), then you can easily convince yourself that the intervention “worked”, and you’ll be inclined to do it again. Conversely, if you use it in somebody who was going to die anyway, and they die regardless, then you can easily convince yourself that you “tried everything”, and you’ll do it again.
“ We do it for drugs, …”
Don’t think so, not anymore.