
Friday Reflection 30: Thirty Years and Counting

SS was a 78-year-old man whose chief concern was simply, “I am dying.” During three visits to his home, I was unable to find anything concerning, or to reassure him that his health was good, or to convince him to come to the office for a more traditional evaluation. Four weeks after our last visit, his wife called me to let me know that he had died in his sleep.
“If the patient tells you she thinks she is dying, take her seriously.” That was the advice I received from a wise attending during my internship. To my ears now, it does not seem like terribly profound advice. It stood out to me because so much of what I’d been taught was more aligned with “trust your gut.” Over the years I’ve realized that both patients and doctors can sense that the end is near. Sometimes the future is obvious, often it is not; sometimes the doctor and patient foresee the same future, sometimes they do not.
As an EBM and diagnostic reasoning obsessive, I often see this as a 2X2 table with the patients knowledge in the columns and the doctors as the rows:
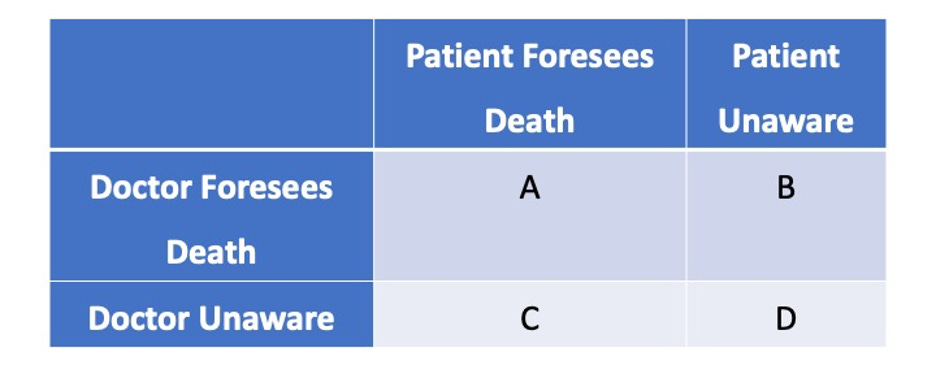
Most commonly, both doctor and patient know when the end of life is near — square A. They agree that it is time to change focus from therapy aimed at cure or slowing disease progression to care aimed at comfort and dignity. These have been some of my saddest office visits, ones in which the patient and I know that this is the last time we’ll be seeing each other. Sometimes we are initiating hospice; other times the patient is moving to be with family who will take responsibility for end-of-life care.
Occasionally, these visits are more difficult and frustrating than sad. MT was an 80-year-old man with pancreatic cancer. Twenty-four months earlier he had presented to a visit with unintentional weight loss. A CT scan made the diagnosis and an MRCP showed that the cancer was unresectable. MT’s multiple medical problems and poor functional status made him a poor candidate for any therapy.
The tumor progressed slowly and, month after month, he weakened but held on. At our final visit he was unable to stand. Although a cliché, he looked like skin and bones in his old loose-fitting clothes. His weight was down about 30% from his initial presentation. He was also jaundiced -- his interventional gastroenterologist was no longer able to keep his common bile duct unobstructed. His daughter, who accompanied him to this visit, and I knew that he could not possibly carry on for long. I am pretty sure MT knew it too. It was the first time I had seen him resigned and sad. That said, he would not hear about hospice care, telling us, and himself, that he might still regain enough strength for the oncologist to treat him. His daughter barely held back tears as he spoke, devastated by his condition, her approaching loss, and the knowledge that his unwillingness to engage hospice was going to make the end harder for both of them.
Two weeks later he died, never admitting he was dying.
If these are situations when both doctor and patient know what is ahead, even when a patient might not choose to engage with the looming reality, there are also times when neither doctor nor patient knows what is ahead. This is what everyone fears, square D.
“He had just seen his doctor and was told he was in perfect health.”
This is a rare situation. Whether due to our testing abilities – we generally know when a patient has a potentially fatal illness – or our ability to risk stratify and offer therapies to prevent instant killers – sudden cardiac death, pulmonary embolism, stroke – unexpected death in the 21st century in someone getting regular healthcare is blessedly uncommon.[i] Yet I can think of a few patients over the last 30 years for whom my conversation with the family began with me asking, “What happened?” Thoracic aortic dissection and PE seem to be lingering threats.
Then there are the situations that fill square B, when the doctor “knows something” but “can’t tell the patient.” I am not referring to a family saying, “Don’t tell grandma she has cancer, the news will kill her.” I think we have moved beyond even considering this an acceptable approach to care. I am referring to situations in which I am “trusting my gut.” I can have a pretty good sense that a patient is dying but lack any definitive diagnosis. I can’t very well tell someone, “I am worried you’re dying but I don’t know from what and thus I don’t think I can help.” In these situations, my approach is a frantic search for a diagnosis. Certainly, this would be inelegant medicine if it happened frequently. But done rarely, by a doctor with good diagnostic calibration, I can defend myself saying that this is part of the art of medicine.
I can think of three patients who fill the “doctor knows the patient is dying and can’t tell” category. For each of them, their final year was filled with a frenzy of consultations, calls to come for another evaluation after I was awakened with a new idea, or hospitalizations for observation and diagnostics. All three died without a clear cause. Each family declined an autopsy.[ii] For only one do I think I figured out the cause of death, retrospectively.
Although I felt I could never tell these people that I thought they were dying, not knowing what was killing them, it is a bit presumptuous to say they did not know. They may have had as good, if not a better, sense of what was ahead than I did.
And now we return to SS. After 30 years, he remains the only patient I have ever cared for who was sure of his imminent demise while I was sure he was mistaken. He is the lone occupant of square C.
This man was a brilliant and famous professor. When I met him, he showed me binders of color-printed (rare at the time) spreadsheets and graphs of his vital signs and physiologic measures. He told me these proved he was near the end. I wish I had paid more attention. I’ll admit that I considered this near-delusional rambling, especially when I factored in his lack of symptoms and normal physical exam. Over the years, as I have learned more about his career, his discoveries, and his approach to problem solving, I would give quite a bit to relive those visits to his home or have another look at those notebooks.
[i] I am, of course ignoring accidents, violence, overdoses, and a new, troublesome infection that led to sudden deaths of many people every year.
[ii] I was disappointed that I would not have an autopsy offering the chance of diagnostic closure, but I also understood that, by the time of death, families were exhausted.
Thanks. Insightful. I hope to know and for my doctor to know. Healthy at 80, I feel I have had my share of life and am thankful for it; I hope to have more and not painfully more.
The combination of being an EBM/obsessed diagnostician (Dr. House?) and landing on quadrant B without evidence must be quite disconcerting! As a student of human behavior, I think it's fascinating the myriad ways people cope with existential matters, and those who work with the dying say that we tend to face death in the same manner we face life, or as somebody put it, "The way we do one thing is the way we do everything." I'm working on the way I do everything, in the hopes that by the time I face death, I've finally got it right!