
Good Ideas Need to Pass Muster in the RCT
The implantable loop recorder is pretty amazing little tool. It provides a lot of data. But data are not outcomes. And, as it turns out, reducing outcomes is not so easy.

Here is a typical scenario: patients with heart failure have frequent periods of acute congestion wherein fluid can accumulate in the lungs and periphery. These exacerbations often require hospitalization for intravenous diuretics and other measures. A hospitalization for heart failure is a negative outcome. Not only is it a buzzkill for patients, its costly and associated with worse outcomes in the future.
Everyone agrees that reducing hospitalizations due to heart failure is a good goal. One way is to have patients be mindful of things like weight and presence of swelling; they can then be taught to give themselves extra diuretics to alleviate the congestion. This however requires a quite skilled and motivated patient. I’d be lousy at it.
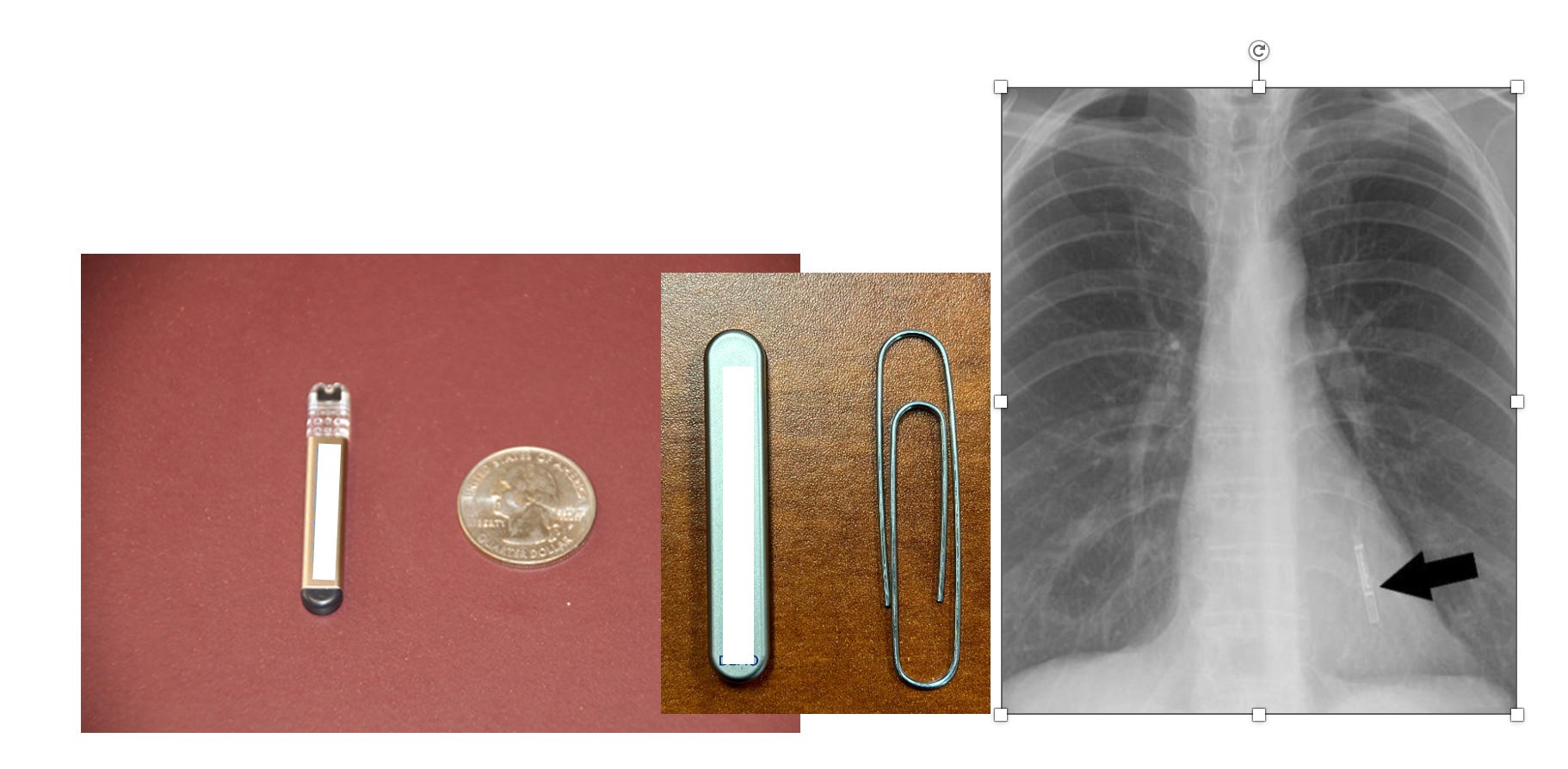
Here is an even better idea: place a little insertable monitor under the skin in the left chest. It’s tiny and takes only seconds to implant. That device has a fluid sensor capable of real-time transmission to clinicians who can act on the numbers to head off congestion episodes.
Here are some images of an implantable loop recorder:
The trial was called ALLEVIATE-HF (Algorithm Using LINQ Sensors for Evaluation and Treatment of Heart Failure) and it sought to assess the safety and efficacy of the Reveal LINQ (Medtronic) ICM with investigational HF risk-status software to guide individually protocolized interventions in patients with HF.
By testing a structured care pathway, this trial represented a pivotal evaluation of the surveillance-driven management paradigm.
A total of 711 patients received the device and were then randomized to active management vs standard care. The intervention was an individualized 4-day as needed increase in diuretic prescription. A prespecified algorithm was set in motion when the device alerted the care team that fluid levels were elevated. Specially trained nurses first ruled out any confounding medical condition or patient safety issues before imitating the higher dose diuretics.
In sum, this was a highly technical substitute for a patient seeing he had gained 5 lbs. and his belt got tight, so it was time to take some extra tablets.
The primary outcome was a 5-component hierarchical composite including cardiovascular death or HF hospitalization or outpatient HF event within 60 days of high-risk onset, Kansas City Cardiomyopathy Questionnaire Clinical Summary Score, and 6-minute walk distance, analyzed using win ratio.
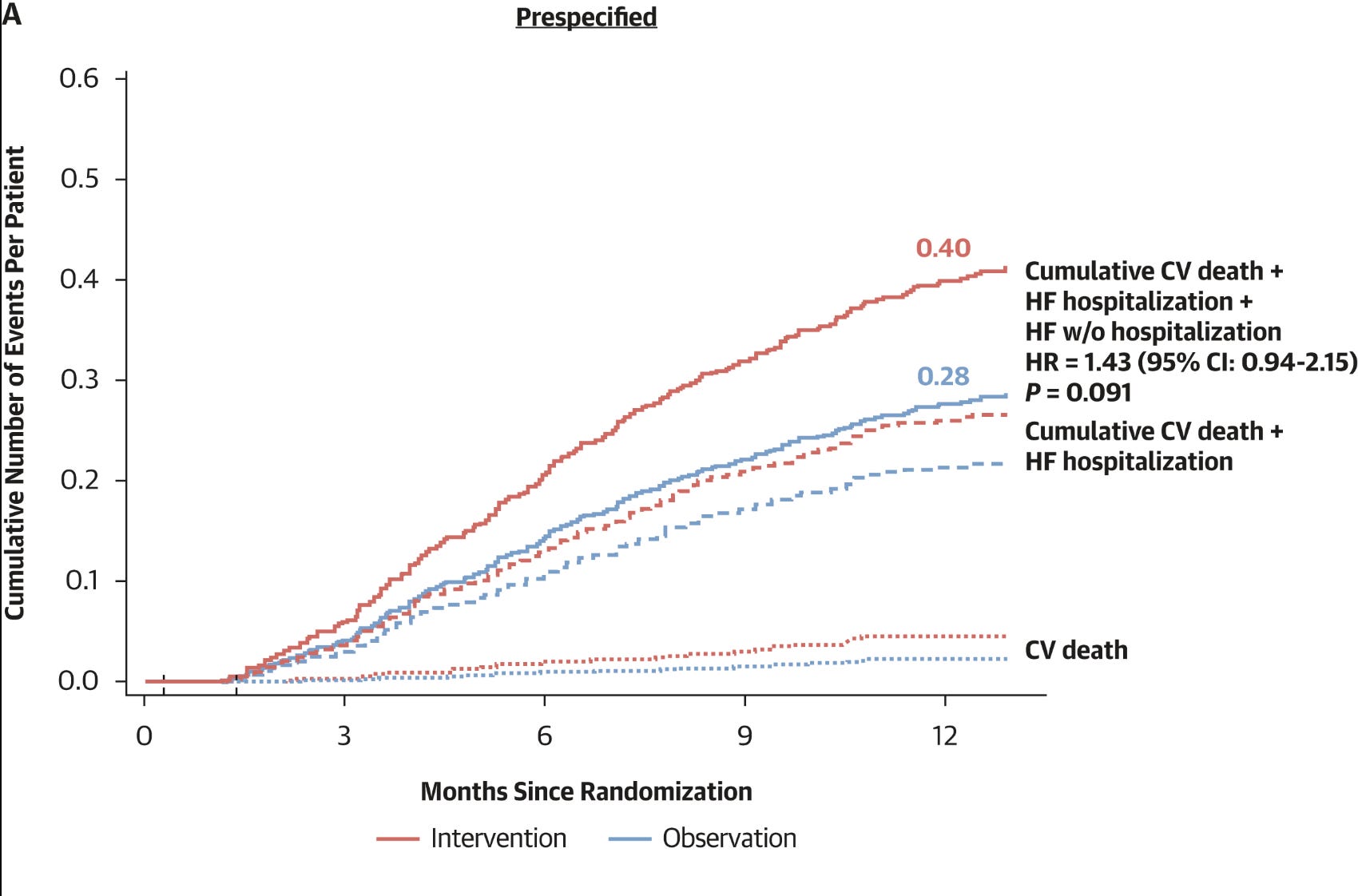
JACC published the study results to little fanfare last week. Why? You guessed it: the trial was negative.
The primary composite endpoint did not significantly differ between groups (win ratio: 0.79; 95% CI: 0.62-1.01; P = 0.06). Win ratios should be positive. This was not. Actually, rates of CV death and HF events were 43% higher (133 vs 93) in the intervention arm.
The authors spent 1900 words in the discussion explaining how and why this result was clearly negative. I can explain it with four words:
It does not matter.
The reasons why or how this good idea failed is not relevant.
I was in Denmark last week to speak at the Danish Cardiac Society meeting in Nyborg. I had many great conversations with Danish doctors. One topic that came up was the implantable loop recorder. We use bunches of these devices in the US. The Danes use almost none.
Why? Because in Denmark, healthcare is paid by taxpayers, and government authorities do careful analyses of cost and efficacy. Their conclusion on implantable loop recorders is that they are a) costly and b) have little impact on health.
Here in the US, I call the devices cash machines. They have an outsized reimbursement for implant—which belies common sense because they can be injected under the skin with local anesthesia in 3 minutes. No sedation required. It’s the easiest procedure you can imagine. But that’s not the half of the cost issue: now, the patient is billed every 30 days for a download of the data. The doctor and hospital receive money every month—like a cash machine.
The current indications for using these devices have been detection of AF after a patient has a stroke, and detection of causes of infrequent fainting. Neither indication has any RCTs showing benefit.
The use in stroke is especially dubious with the new knowledge that short-duration AF episodes are common and associated with lower stroke risk than clinical AF detected with symptoms.
The companies who make these little cash machines wanted to expand their indication. And since they can also be equipped with a fluid sensor, the idea came to use them to help adjust medications in patients with heart failure. That was the origin of the ALLEVIATE HF trial. But it failed.
The answer is simply don’t spend dollars on these devices for this indication. Good, we learned something from ALLEVIATE HF.
The trial makes the Study of the Week for multiple reasons: one is that all good ideas require testing in RCTs. And not all marketing studies turn out positive.
Yet will need to be on alert, because negative marketing studies don’t often die peacefully.
On the same day that the authors published negative results, comes a post-hoc analysis from the trial showing that the recorder placed for managing heart failure also detected arrhythmias, and some of them were bad, and required interventions.
The authors spent another 1800 words explaining this finding with the implication being…maybe we should still insert these cash machines because even if they don’t help manage heart failure, they pick up arrhythmias.
Of course, this would be a foolish conclusion, because to test that conclusion we would want a separate trial with its own prespecified primary endpoint. You can’t change endpoints after seeing the data.
Footnote: Thanks for all the new subscriptions. We appreciate your support and have big plans to expand Sensible Medicine, including recording more educational videos this summer. JMM
Again, a triumph of technology over reason. An electronic scale and FaceTime and a nurse is worth a room full of cardiologists. Practicing in Lampasas small town we would have the elderly people come back who didn’t have family to check on them more frequently. They almost didn’t need to be seen. They just needed to walk into the waiting room to have the nurse eyeball them and their feet and send them on their way. The intravascular implantable pressure monitors seem to at least have a medical reason why you might pick up changes before you see the edema. A story involving my dad -at age 96 -he gets admitted in September 2024 hypertensive heart failure troponin of 10. Gets usual IV lasix drip. Moves closer to our home goes into assisted living and now gets the usual decent medical therapy. He weighs 190 down from 240 has zero edema. PT says he can walk 1600 feet with his WALKER do the math on that-still in slow a fib on anticoagulation. He has had no hospitalization for heart failure other things but not heart failure for two years. What changed?
Nursing care , son to check on him in person; meds handed to him daily and the lack of a car to go to Dunkin’ Donuts and McDonald’s. The the latter is probably ranked the highest.
Excellent as always. Another proof to what I’ve been teaching my trainees for years, “the heart is too important an organ to be left to a cardiologist.”