
Good Ideas Require Testing – The Lessons of the NUDGE CKD Trial
Policy interventions can affect more people than specific treatments; they should also have to pass muster in randomized trials

Kidney disease does not get the attention it deserves. Heart disease and cancer suck up most of the attention. The kidney is complex (without a simple clogged-pipe frame). Kidney disease progresses slowly, often with overlap from heart disease.
But end-stage kidney disease requiring dialysis affects more than 2 million people, and patients on dialysis have 5-year survival rates of only 50%. Chronic kidney disease (CKD) if left untreated may progress to ESKD.
Kidney disease seems like a great target for prevention. And… we have two drug classes that have been shown to slow the progression of kidney disease. Yet, in my clinic, I see few patients with CKD who are taking either of the two classes of medicine shown protective--renin-angiotensin system inhibitor (RASi) or a sodium-glucose cotransporter-2 inhibitor (SGLT2i).
I often send notes to primary care clinicians (or patients) to consider discussing one of these drug classes. Patients, too, often know little about a) the condition of CKD, and b) that there are treatments. Empirical data support the sorry state of patient knowledge regarding kidney disease.
Here is a really good idea: to increase usage of CKD-protective drugs, we send letters to patients and clinicians. Surely these educational nudges will help increase the usage of beneficial medicine.
NUDGE-CKD Trial
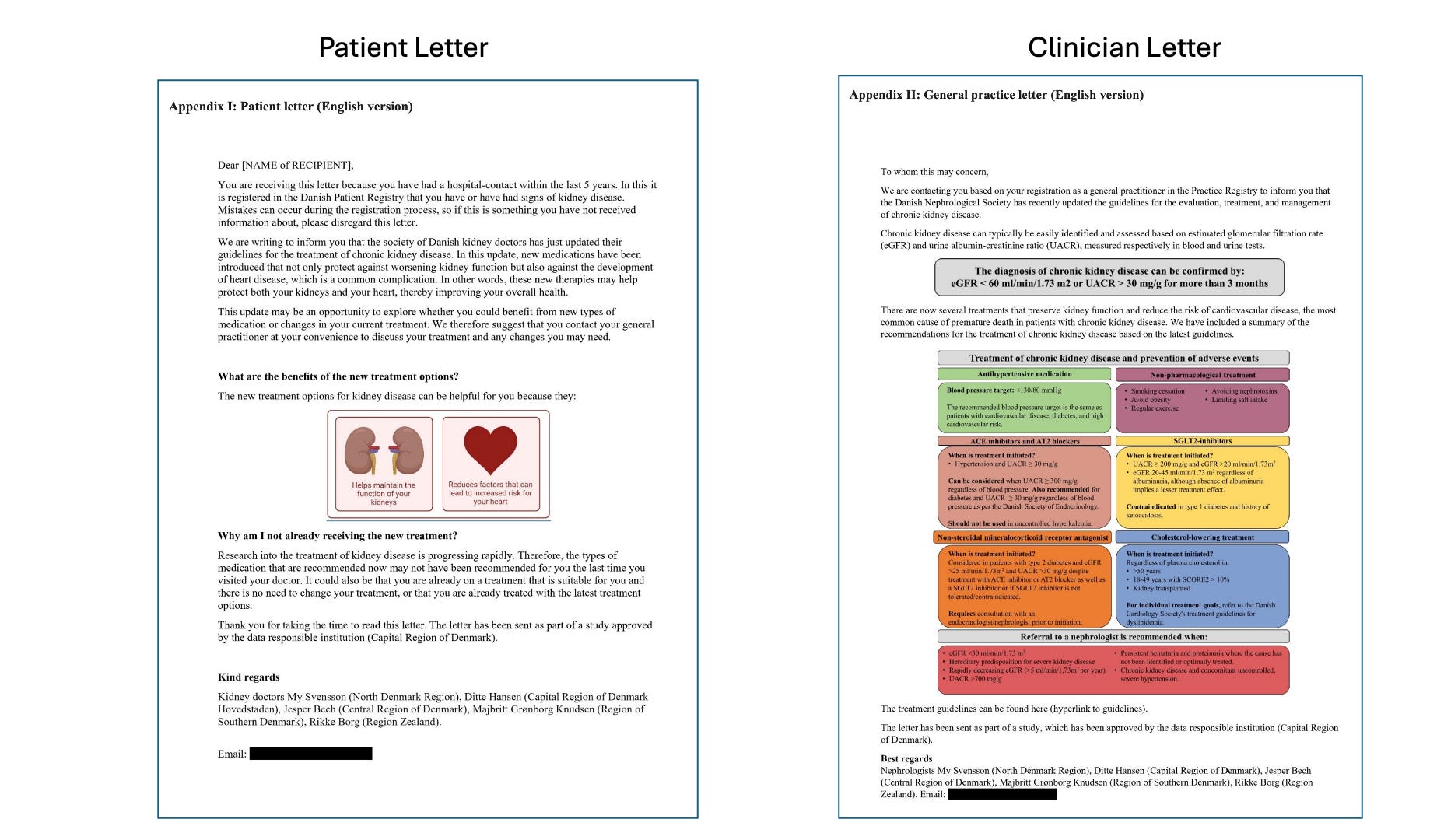
Danish investigators decided to study the nudges, which were one-page educational letters designed to provide knowledge of disease and treatment. Here are the letters.
In Denmark, patients and their clinicians receive government letters via email. This allows randomization to receive or not receive notifications. The DANCAVAS cardiac screening trial used this method to study being invited (or not) to cardiac screening.
In NUDGE-CKD more than 22,000 Danish adults with hospital-diagnosed CKD were randomized to the patient-level intervention, and ≈ 1,500 general practices caring for 28,000 CKD patients were randomized to the provider-level intervention.
The primary endpoint was a filled prescription for either a RAS inhibitor or an SGLT2i within six months. This, too, could be assessed via the national Danish registry.
The results were clear and informative
In the group of patients who received a letter, 65.1% filled prescriptions vs 65.9% in the control arm. The less than 0.8% difference did not reach statistical significance.
For patients with providers who received letters, 63.9% vs 64.4% in the control arm received prescriptions. This tiny difference did not reach statistical significance.
One reason why the letters may not have worked is that patients did not read them. This was not the case for Danes. More than 80% of patients reported reading the letter and 81% had a positive attitude about receiving similar updates.
The authors spend a great deal of time explaining why this simple but elegant intervention did not work. Maybe the letter wasn’t detailed enough; maybe the patient and doctor’s notifications were not synchronized, or perhaps too many of the patients already had specialty care. They cited other nudge-type studies that had modest positive effects, but required more resources.
My Comments
I cover this important trial for multiple reasons.
First, we learn just as much from negative as positive trials. That the simple nudges did not work is important knowledge. Scientists should not be deterred from studying truly unknown questions. Too many studies are simply designed to show something (usually a drug or procedure) works.
Second, sending letters to patients and clinicians about their disease is a policy intervention. It’s a good idea, steeped in beneficence. But policies can affect many more people than specific treatments. That makes it crucial to study these interventions in randomized trials. Imagine a world in which the failed hospital readmissions reduction policy was studied in an RCT before it caused harm.
Third, when it comes to prevention of chronic illness, I don’t believe there are antibiotic-like gains coming in the near future. We are unlikely to have a miracle cure of type 2 diabetes, or chronic kidney disease or hypertension.
One of major areas of progress going forward may be to maximize the number of people who benefit from proven therapies. This goes by the awful name of implementation science. It’s not as exciting as discovering that ACE-inhibitors and spironolactone shred mortality in heart failure. But it is what it is.
I love this effort. The Danish investigators deserve praise for showing policy-people the importance of testing good ideas. Because being a good idea does not equate to benefit.
Brother I hear you loud and clear. However, while ACE/ARB's widely available cheap. Sodium-glucose cotransporter-2 inhibitor (SGLT2i) not so much even though FDA has approved them to be manufactured. At least not that I have seen.
Typical Pharm industry greed. The whole industry is counting on Atheism and no repercussions in the next life, as it is obvious they have no shame in this one.
Cheapest I can find is over $500 without having to fill out bullshit begging for cheaper drugs to get in the pharm program to get for lower price that is still quite steep
I would add GLP-1s to the list of agents shown to reduce progression to ESRD in patients with diabetes and obesity. Obviously, GLP-1s come with a hefty price tag. When RASAs and SGLT-2 inhibitors are underutilized, a scenario where GLP-1s are preferentially utilized, is not unimaginable
Most of us don’t get to practice or get care at a Kaiser, a Sentra or an Intermountain. In an era of fragmented EHRs, an integrated system is our best bet at driving up adoption of these life (and kidney) saving meds