
Guidelines, Evidence-based Medicine, and the Practice of Medicine
A meandering meditation on the flaws of guidelines and how evidence often barely affects practice

On March 13th, the 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia was released.
On March 27th, I saw CW, a 60-year-old man with an LDL cholesterol of 224 and CAC at the 52nd percentile.
I’m a total EBM devotee. EBM gives us the best chance of practicing effective, patient-centered, parsimonious medicine. EBM is the process of integrating clinical experience and expertise with the best available evidence from systematic research. EBM tends to de-emphasize intuition, unsystematic clinical experience, and pathophysiologic rationale as sufficient grounds for clinical decision making. EBM stresses the examination of evidence from clinical research.1
EBM has its shortcomings, many of which were predicted by Alvan Feinstein. Feinstein was a product of the University of Chicago, receiving a bachelor’s in 1947, a master’s in mathematics in 1948, and his MD in 1952. Although we will, of course, claim him, he made a name for himself at Yale. He was a giant in the field of clinical epidemiology and a founding editor of the Journal of Clinical Epidemiology
Feinstein was a skeptic of EBM from the start. He noted that a minority of clinical decisions can be addressed by RCTs – the ultimate source of truth in EBM. He argued that EBM mostly focuses on hard outcomes, while most of medicine focuses on improving soft, difficult-to-measure outcomes. For me, he was most articulate at highlighting that the evidence generated in studies is for an average patient, one who does not exist. The patients we care for, like all of us, are unique. Two patients might have the same disease, or risk factor, but they differ in the severity of their symptoms, their co-morbidities, their genetics, and everything we pay attention to in the past medical, social, family histories, including previous treatments and treatment trials, ability and interest in adhering to therapy, functional status, and on and on.
Clinical practice guidelines, which have only become important since the passing of Feinstein in 2001, grew out of EBM. Recommendations come with a strength and a quality of evidence. The strength of a recommendation considers the balance of benefits and harms, while the quality is based on the type of study supporting the recommendation.
The pros and cons of guidelines have been discussed endlessly. The longer I spend with them, the less of a fan I am. I understand that they help standardize care, and they certainly make it easier to find basic recommendations on things you know little about. But the more I read, the more I feel that guidelines are overly influenced by people with either financial or intellectual conflicts of interest. The power on the guideline writing committees is seldom held by experts in research analysis, but rather by content experts. Too many recommendations are “strong but based on weak evidence.” This is how we parent, but it should not be how we practice medicine. I also see trainees relying on guidelines and not thinking enough about the patient in front of them
I have finally finished reading the new cholesterol guidelines. I don’t think Feintstein would be surprised by how divorced they are from any consideration of value. As noted, a strong recommendation is given when the benefits of a treatment far outweigh the risks. In the cholesterol guidelines, we are mostly talking about statins, exceedingly safe drugs. Thus, most recommendations are strong. This figure is telling.
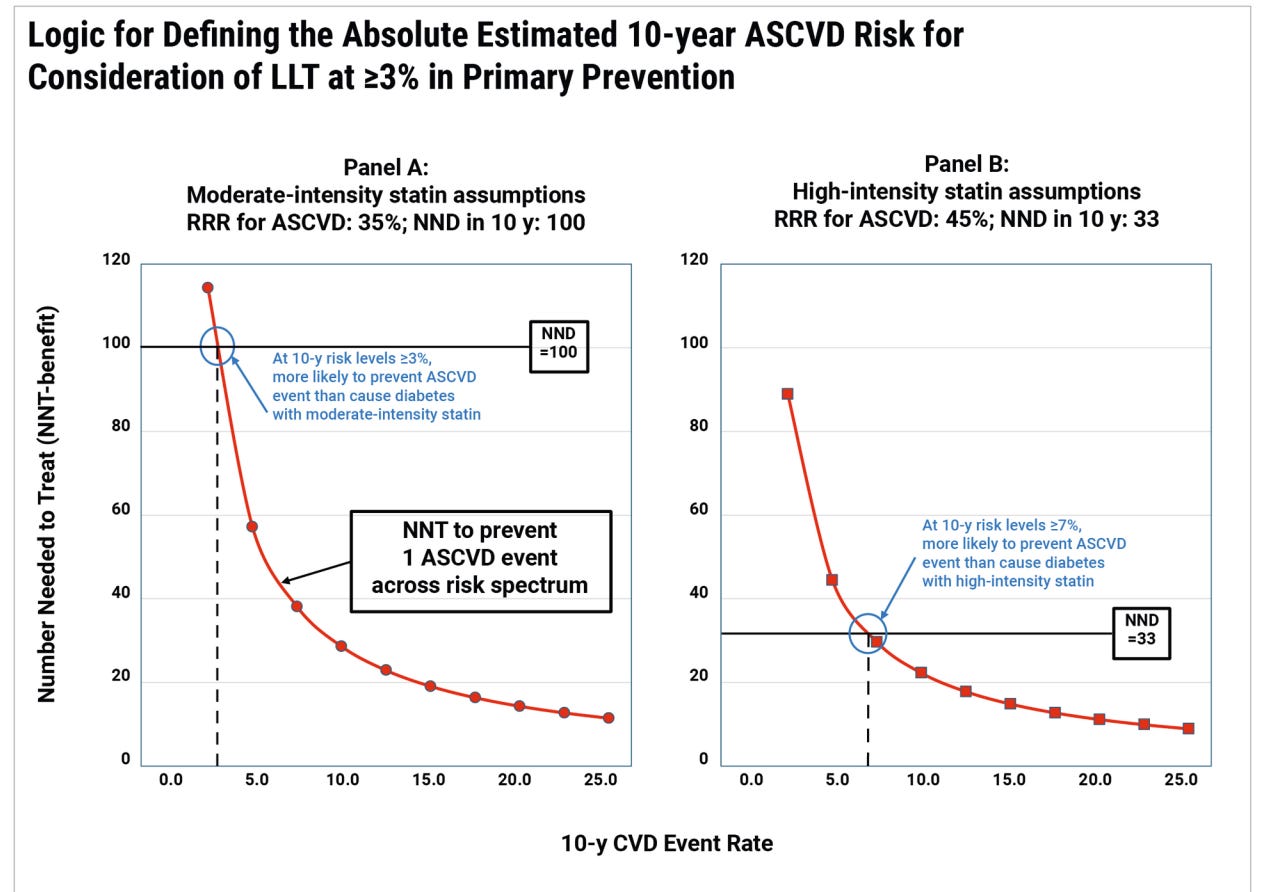
The authors define treatment threshold based on one side effect that could be quantified, the balance of cardiovascular benefit against the likelihood of incident DM. These are not equivalent, or even comparable, outcomes. They neglected to consider so many things. There is the cost of the medication, the monitoring, the visits, and the turning an enormous swath of the population into patients. Treating a patient with a statin who has a 3% 10-year risk might reduce the risk to 2% — helping someone with a 97% chance of doing well reach 98%. Is this how we want to spend our time, our effort, and our money?
Of course, the guideline suggests shared decision-making.
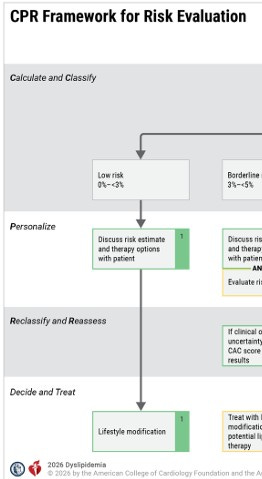
With a different value set, a different view of medicine, you could imagine the guidelines being a fraction of their 134 pages. If we concentrated on treatment and only the highest yield prevention, the guidelines would focus on secondary prevention and primary prevention in those with familial dyslipidemia. I recognize this might sound like the ramblings of a crazed minimalist — heck, I am not even sure I agree with myself — but it seems less crazy when you see algorithms that include this:
If we are serious about spending less money on healthcare AND getting better outcomes, we might start by thinking seriously about the actual clinical effect of the money we spend.
Let’s get back to CW and Dr. Feinstein. CW adamantly refuses to begin a statin. The irony of seeing CW on the day I read the guideline was glaring. Anyone familiar with preventative cardiology data would agree that he should be on a statin. However, given his “Feinsteinian clinical nuances,” he is utterly unaffected by evidence or guidelines. There are certainly people who err (my value judgment) in the other direction, people more aligned with the guideline writers, those with a 0-3% 10 year risk who choose to take medications (as long as they are not directly charged for them) or change their lifestyle for the possibility of a 1% risk reduction.
When I think about how EBM actually affects my practice, I recall this figure from a 2024 Sensible Medicine post by Mariana B. Caiado Ferreira.

I could re-label this diagram like this:
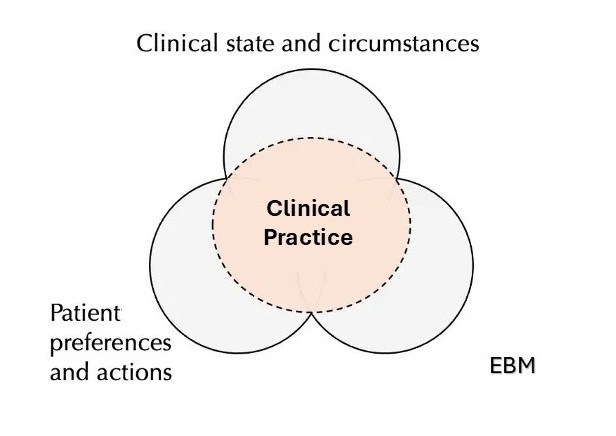
My practice depends on my practicing EBM but, most of the time, my patients’ clinical state, circumstances, preferences, and actions crowd out EBM. I often end up doing something only vaguely related to the studies or the guidelines.
These definitions are almost plagiarized from something written in the late 90’s, probably by the McMaster people. I have been using them in talks and handouts for years and don’t know where they originated.
I think this is a great perspective and illustrates the tension we face when trying to practice EBM.
I share your feelings about guidelines in general—I wrote fairly critically of cancer screening guidelines last September. However, I think that guidelines can and should have a place in medical practice.
Most practicing clinicians will never be able to keep up with the primary literature on their scope of practice, especially generalists like us. Having a panel of experts parse out the evidence and distill it down to something actionable makes a lot of sense. But the authoritative epistemic posture of guideline panels today is a major problem.
“We’re experts so you should do what we say” isn’t (and shouldn’t be) acceptable with the level of distrust in the medical field today. As I argued in my screening guideline essay, guidelines would serve clinicians better by equipping rather than directing. Teach the uncertainty and nuance in the evidence and use clear statistics such as NNT and NNH so that practicing clinicians can more easily apply them to individuals. The blanket approach to recommendations is a disservice, especially when the evidence is weak.
I would also prefer to see simpler guidelines that focus only on the interventions that improve meaningful outcomes based on high-quality evidence. Making what should be a ten page document into a few hundred puts it out of reach for most. Standardize practice around the best evidence. We don’t really need to make recommendations about every obscure item in the topic. Find another document in which to publish that.
Anyway, sorry about the mini-essay in the comments—you got me thinking too much this morning!
It has been obvious for years that guidelines absolutely cannot be trusted in any medical category linked to politics - any guidelines regarding transgender care, or dealing with vaccines, for instance. Unfortunately, you also can’t trust guidelines linked deeply to new sources of major pharmaceutical profits - ADHD ones, or weight loss ones. But I always figured that the legitimate, respectable, apolitical old fields, like say cardiology and oncology, were trustworthy - then I started reading y’all and learned from Vinay that oncology is full of garbage studies and from you that cardiology is full of garbage studies. Moral of the story: I’m sure at least all the asthma guidelines must be faultless! ; )
Much, much more on the profound flaws of guidelines and the inevitable death of human medicine here:
https://gaty.substack.com/p/the-three-wise-men-walk-into-a-doctors