
How Doctors are Fooled
For the next few weeks I will explore the need for having a proper control arm in medical studies

Two major studies presented this weekend at the American College of Cardiology meeting may herald new ways to treat two common cardiac conditions. Yet the foundation of these new approaches rest on dubious evidence.
This starts a multi-part series exploring a common theme in these studies—the control arm.
This first week I will tell a story from my first years of private practice.
Next week, I will explore a study of treating patients with valvular heart disease without open-heart surgery. The authors report the results as “positive,” but the control arm figures in how we interpret the results.
The following week, I will write about the use of an older medicine for a new condition, which may or may not exist, depending on how you think about control arms in studies.
During the first week of my first job as a doctor, at Audubon Hospital, on Poplar Level Road in Louisville, KY, I read the chart of a man who was Day 2 after TMR.
I asked Kim, our rounding nurse, “what is TMR?”
She said, “it’s transmyocardial revascularization—a heart surgeon opens the chest and lasers many holes in the ventricle. It’s done to relieve angina. You’ve never heard of it?”

TMR was a big deal. It required open chest surgery. It took patients many days to recover.
I was baffled. Just weeks before I had finished a top training program. During those years, I had moonlighted at a busy private cardiology group. I had never heard of TMR.
But at Audubon hospital, up on the hill on Poplar Level Road, TMR was common. I asked my partners about it. “John, I know, it seems strange, but patients feel better after it; their angina gets better. We see it.”
I shook my head and carried on. Google did not exist. There were no cell phones to look up studies. There were no private message groups to pose a question to.
And…
It turns out that in the NEJM in 1999, a study comparing TMR to medical therapy in patients with severe angina due to coronary disease found the following:
In the first year of follow-up, 2 percent of patients assigned to undergo TMR were hospitalized because of unstable angina, as compared with 69 percent of patients assigned to medical treatment
So, for years, at Audubon hospital and many other hospitals, patients with severe coronary disease and chest pain had holes drilled into their hearts to improve blood flow. All of these patients faced a long recovery; some had serious complications and even died from the procedure.
Then. Boom.
Nine years later, a group of investigators finally decided to study TMR in a proper way: they included a group of patients who had surgery but did not have holes placed in the heart. We call this a placebo or sham control.
These are charts from the paper.

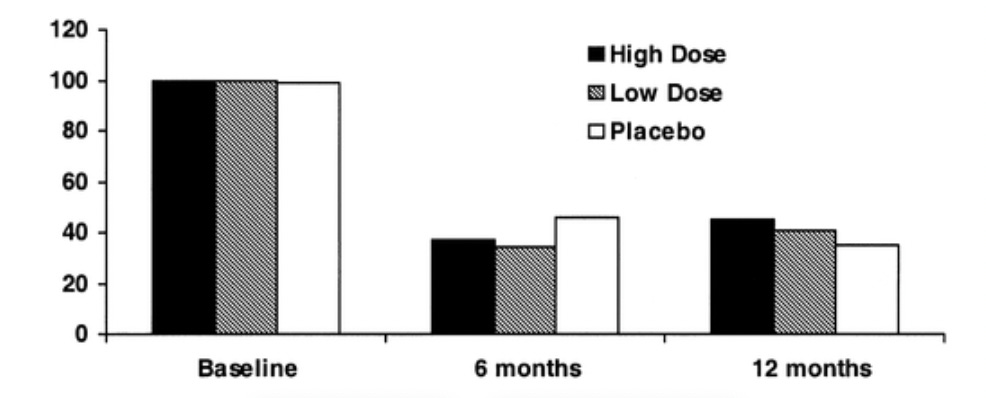
The pictures clearly show no difference in exercise capacity or angina in any of the three groups. High-dose laser, low-dose laser, or no laser all had the same results.
Opening the chest of patients and lasering holes in the heart did not work any better than a sham.
And that was it for TMR. It was all placebo effect.
We never did TMR again. We sort of forgot about it.
How Were We Fooled?
Earlier studies of TMR against medical therapy plus our experience with patients who felt better after TMR plus the eminence of the surgeons who advocated for the procedure had utterly fooled us.
This happens when you compare a huge procedure (surgery) against something small (medicines); patients tend to feel better after a bigger procedure.
Placebo effects are super-complicated. But they are real. It’s why drug trials use a placebo pill.

This history of medicine is replete with examples wherein a proper control arm reverses a practice. Brian Olshansky, MD, wrote this wonderful review of placebo and nocebo effects—it is open access.
Finally…
It might seem unethical, bordering on barbaric, to operate on a human and not do the surgery. The flip side, however, is the ethics of doing ineffective invasive surgeries on hundreds or thousands of humans—for years.
Tune in next week and I will discuss the big study on treating valvular heart disease without open-heart surgery. Control arms take center stage.
John,
I remember having to cover the OR TEE service at Audubon hospital on occasion and finding myself involved in a bizarre procedure I had never encountered before. During these TMR procedures I was instructed to yell "hit" when micro bubbles appeared in the left ventricle. It seemed ridiculous that I was doing this and I was shocked that my colleagues were referring patients for the procedure.
At the same time we were running EECP beds, a noninvasive (but time-consuming) procedure for refractory angina which had little supportive evidence from placebo-controlled RCTS. But patients definitely felt better and studies to this today confirm this improvement which is likely due mostly to placebo effect (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7273423/)
Anthony
How timely an article...how were the doctors fooled about this cardiac procedure? Oh please, can we expand into this COVID exercise with doctors stating falsehoods too..to their patients...a safe and effective “vaccine”...and that HCQ/ivermectin are BAD...How about...minimal addiction from those new strong opiate drugs several years ago. These are the days of the Big Pharma influences at the very top of the medical food chain...Congress and thru the FDA...political control most evident of the very people who treat US....more like medical political officers now. I greave for medicine of the past...where training was truly interested in a doctor-patient relationship built on trust...too many doctors still think this “vaccine” is safe and effective.