
How to Keep up with the Medical Literature

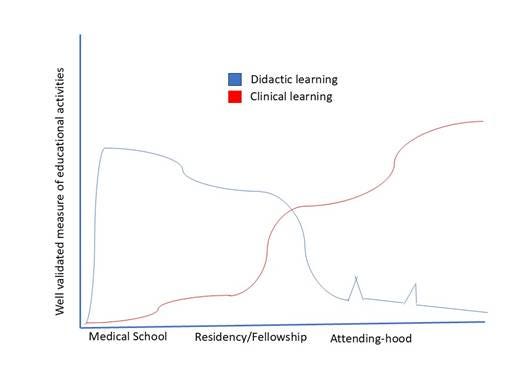
Medical education begins as an exercise in didactic tolerance. You sit through lectures, study textbooks (or the 21st-century equivalent), and listen to your more senior colleagues telling you what to do. Then, little by little, and eventually all at once, you become responsible for your education. Once you are out of training, you learn by reading about the patients you see – either those in front of you or those you’re likely to see in the future. You read journal articles, reviews, and guidelines. Occasionally, you learn something at a conference, but this is rare.
Keeping up is hard because there are so many things competing for your time. Ignore the journals for a week, or a month, or a year, and you (and your patients) are likely to be fine. But continue to ignore incoming information, and you will fall behind. The promise of a “review course” that will get you “up to date” is as false a promise as the latest from a longevity guru.
Everybody finds their own way to keep up. Here are some suggestions to consider. I’ve also included what I do as an example (understanding that these apply to a generalist, my patient panel, and my idiosyncratic interests; in other words, they apply to me).
Set Goals
Every job requires a different type of expertise. You need to decide the breadth of knowledge that you need based on who you are and what you do. A department chair once told me that she read the introduction to every article in the NEJM, JAMA, Lancet, and BMJ because this gave her an understanding of a broad swath of medicine. I generally skip introductions. A generalist will read differently from a sub-sub-specialist. Start by defining where you aim for excellence, where you aim for adequacy, and what you can ignore.
For me, I go for detailed knowledge of articles that will immediately affect my practice. I also look for important examples of medical reversals and, since I am supposedly an academic, I try to maintain a cursory understanding of major trends in the clinical studies from subspecialty medical and surgical fields.
Choose your journals
Start with major journals in your field and then whittle them down as you get a sense for what they publish. You always need to balance breadth and depth. A generalist is likely to skim multiple journals, while a subspecialist may read one or two journals cover to cover. Have the tables of contents of your chosen journal emailed to you. Do not delete the email until you have reviewed the issue.1
I read the NEJM, JAMA, and JAMA IM pretty closely. I look at the titles of BMJ, Lancet, and Annals of Internal Medicine. Even doing this, I miss a lot of interesting articles. This is where Twitter and reading John’s Study of the Week come in. They help me to catch articles I would have otherwise missed.
Skim effectively
Nobody can read every article with the attention I give to the two articles we cover every other week on Fortnight. Thus, you need to learn to effectively skim. Effective skimming requires you to use abstracts to do an initial appraisal of an article to determine if it is worth reading. My suggestions (biases included):
For RCTs, consider whether the results, positive or negative, might change your practice. If so, is the study large and the endpoints clinically robust?
I almost never read cohort studies unless the results are truly surprising; they will not change my practice, and there is only so much time.
I think case-control studies are worth reading if the topic is important and the odds ratios are large.
There are not enough diagnostic test (or clinical decision rule) studies. When one is published, I use the abstract to determine whether the test is usable and whether the study’s design limits spectrum and verification bias.
When I skim, I read all the titles and the abstracts of articles that seem clinically useful. If an article is worth reading, I skim the intro, read the methods, figures, tables, and the results. I do not read discussions. I read editorials if I am confused. I only closely read articles that will change my practice or that I plan to write about, talk about, or teach from.
Summary tools
There are many good summary tools out there: Journal Watch, ACP Journal Club... I have colleagues who use these effectively. I have never found them very useful, as they seem to feed me more articles rather than more important articles.
Colleagues
I find colleagues invaluable sources of information. I ask them questions. I eavesdrop when they talk about topics I don’t know enough about. Throughout my career, I have found it useful to review journals with a group. When we were most organized about this, we met once a month. Each member of the group was responsible for one journal. Important articles were summarized on a single, highly structured page. The task of summarizing and discussing an article helped me to retain the information.
On-the-go searches
It’s rare that I don’t need to look something up. UpToDate and OpenEvidence are my go-to, in-clinic resources. They are great for answering a question, but learning about a topic takes more time. I make sure to return to the page later in the day. I usually print a few key papers to read.2 If there is one absolute truism in medical education, it is that you learn best when the topic is associated with an actual patient. I remember everything I learned about cirrhosis, caring for JR in medical school. I remember little of what I read in JAMA last week. In the last six months, I have completely retooled my knowledge of the following topics based on the patients I have cared for.
Diagnosis of light chain disease
Prophylactic surgery in people with BRCA mutations
Novel diagnosis tests and treatments for patients with Alzheimer’s disease
Differential diagnosis of renal tubular acidosis.
Conclusion
Keeping up is hard. Lots of people do it well, and everyone does it differently. The only real truism for me is that you learn best when you are reading about a topic that is directly related to the care of an actual patient. Please chime in with your own tricks of the trade.
For the most part, I review articles when they are included in an issue rather than when they are published online. This means I am sometimes behind, but, as they say, it is a marathon, not a sprint.
I know, I know, it is weird; I still like to read on paper.
In 2026, clinicians are more deficient in common sense than factual information. Reading the latest Elsevier, Wiley, Wolters, etc journals would contribute little to practical, useful, or actionable knowledge (Isn’t at least half of published research either wrong or outdated in a few years anyways)?
For 99% of practicing clinicians in the trenches, they’d be better off reading textbooks (yes, paper with no ads) to brush up their general knowledge, use AI tools like OpenEvidence, and read plenty of books on decision-making under uncertainty (ie Kahneman, Klein, Taleb, etc).
I am not a medical professional, but I spent my career as a librarian/information professional. May I suggest that one way to keep up with some of the literature is through the NLM's National Center for Biotechnology Information (NCBI). You can set up searches for whatever diseases, conditions, techniques, etc. you want and you'll receive a daily list of links to new articles, previews of articles to be published, and more that are newly referenced in PubMed. I've found the lists to be very focused and very helpful to me as a patient who is interested in new research in a specific area.