
I Am Afraid of Early Cancer Detection
Part II: All the reasons I am afraid

Last week, I wrote about Grail’s Galleri test, a test marketed as a single blood test that screens for 50 cancers. Last week’s article outlined my pretty dim view of the test. I referenced a Wall Street Journal Opinion piece, Who’s Afraid of Early Cancer Detection?
One answer to the question posed by the WSJ piece is: me.
Why does early cancer detection frighten me?
1. Right now, with our present technology, early cancer detection – which I am using interchangeably with cancer screening - too often fails to improve overall mortality. Instead, it succeeds in yielding overdiagnosis and overtreatment. As a nation, we have embraced mammography, colonoscopy, and PSA testing as part of routine healthcare. Part of my job, as a primary care physician, is to discuss these tests with most patients over 50 (or maybe 45, or maybe even 40). But if you really spend time with the data for mammography, or colonoscopy, or prostate cancer screening, you have to ask yourself, what the hell are we doing? I worry that we are doing at least as much harm as good for our patients (and enormous harm to our health care budgets).
2. If the cancer screening we currently accept as “standard of care” frightens me, then novel screening tests -- whether Galleri or the new darling, whole body MRI – terrify me. We (patients, doctors, developers, investors) do not have the patience required to collect the data necessary to prove these tests decrease mortality. The WSJ piece makes this clear. (Every time I read this paragraph, I grind another layer of enamel off my teeth).
“Requiring randomized controlled trials and FDA approval for multicancer early-detection tests could restrict access for years. Hundreds of thousands of patients would likely have to be enrolled in trials, some receiving the test with the others in a control group. They would have to be followed over many years to determine whether patients who received the test were diagnosed with specific cancers earlier than those in the control group and how much longer they lived as a result. Proving a statistically significant benefit could take a decade or longer.”
A paragraph later:
“Dana Goldman, the University of Southern California’s dean of public policy, likes that idea: ‘There will be a lot of suffering if we have to wait 10 years for the tests to be approved.’”
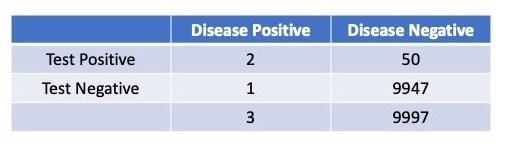
3. Closely related to #2, I am afraid of the cost of this type of cancer screening. Think of the cost to Medicare of every patient who shells out $1000.00 for Grail’s test. Building on my previous example, if 10,000 65-year-old men are screened for pancreatic cancer (grossing $10M for Grail), about 52 people will have a positive test. Two of these men will prove to have disease and, maybe, one will have his life saved. But all 52 will require an evaluation[i]: an MRCP, possibly an ERCP, and probably repeat testing for some time, all to prove that the positive Galleri was a false positive. It’s a good thing the federal government has nothing else to spend healthcare dollars on. (I’ve opted not to spend much time on MRI screening, but research to date suggests it is not much better).
The inequities that calculus guarantees are repugnant. Those with the ready cash to spend $1000 on an unproven screening test end up stealing healthcare dollars from those who need the money to pay for proven interventions, such as childhood vaccination and treatment for symptomatic disease that worsens people’s quality of life.
4. I am also afraid of how this type of screening will affect medicine. Although I don’t like it, I feel a necessary part of the practice of medicine is counseling people on the inevitability of our decline and death. Like all of us, I would love to have treatments for more of the diseases that shorten our lives. But tests and treatments that promise to protect us from the inevitable, diseases that seem part and parcel of the human condition, trouble me. This is why I hope that early detection and cure of late-life cancer or dementia seem empty to me. Call me defeatist, a pessimist, an old doctor who cannot dream of a better future for medicine. I’d rather say I am a realist, both as a doctor and a human.
5. And last, personally, I am afraid of this type of cancer screening because I am afraid of cancer. Without going into too much detail about my own health, I will probably not die of coronary disease. That means cancer is my likely mode of exit. I have never smoked, so lung cancer is unlikely. My PSA is very low, and I do colon cancer screening, so those are unlikely causes of death.[ii] I may very well, therefore, die of pancreatic cancer. I fear being tempted by tests advertised as protecting me from this fate. Tests that my brain tells me are ineffective, dangerous, and -- considering the greater good -- probably unethical, but that my heart (or pancreas) might desire.
Next week, for the 3rd and final installment in this cancer screening series, I will discuss some of Peter Attia’s good, and very convincing, arguments.
[i] The 2X2 table for this calculation:
[ii] Don’t @me about that statement, especially you, Drs. Mandrola and Prasad.
I’d rather shell out $1000.00 for a personal trainer or a chef that can introduce me to new healthy tasty recipes. Real preventive medicine is primarily learning and maintaining healthy habits.
"The inequities that calculus guaranties is repugnant. Those with the ready cash to spend $1000 on an unproven screening test end up stealing healthcare dollars"
And that is exactly what it's all about. The industry is trying to maximize its share among healthcare expenditures.
Medicine is becoming a business. It's been happening for years, but in recent times things really seem to be getting out of hand.
Very good article, thank you.