
I have yet to find a study with more spin
In the past 4 posts, I have shown that systemic RX for stable coronary artery disease (meds) do as well as focal RX (stents). That data had very little effect on actual practice. Why? Watch this:

Regular readers know the deal about medical studies.
In the simplest sense, you randomize patients to two treatments. Random assignment (mostly) balances the known and unknown factors. You declare an endpoint before the experiment and then report that endpoint. There may be secondary endpoints, but the focus is always on the primary endpoint.
I will first present the trial in question without any specifics. Treatment A vs B. The primary endpoint was a composite of death and a very bad event.
Here was the Kaplan-Meier curve of the study in question. The y-axis was the cumulative percentage of the primary endpoint—either death or a very bad outcome.
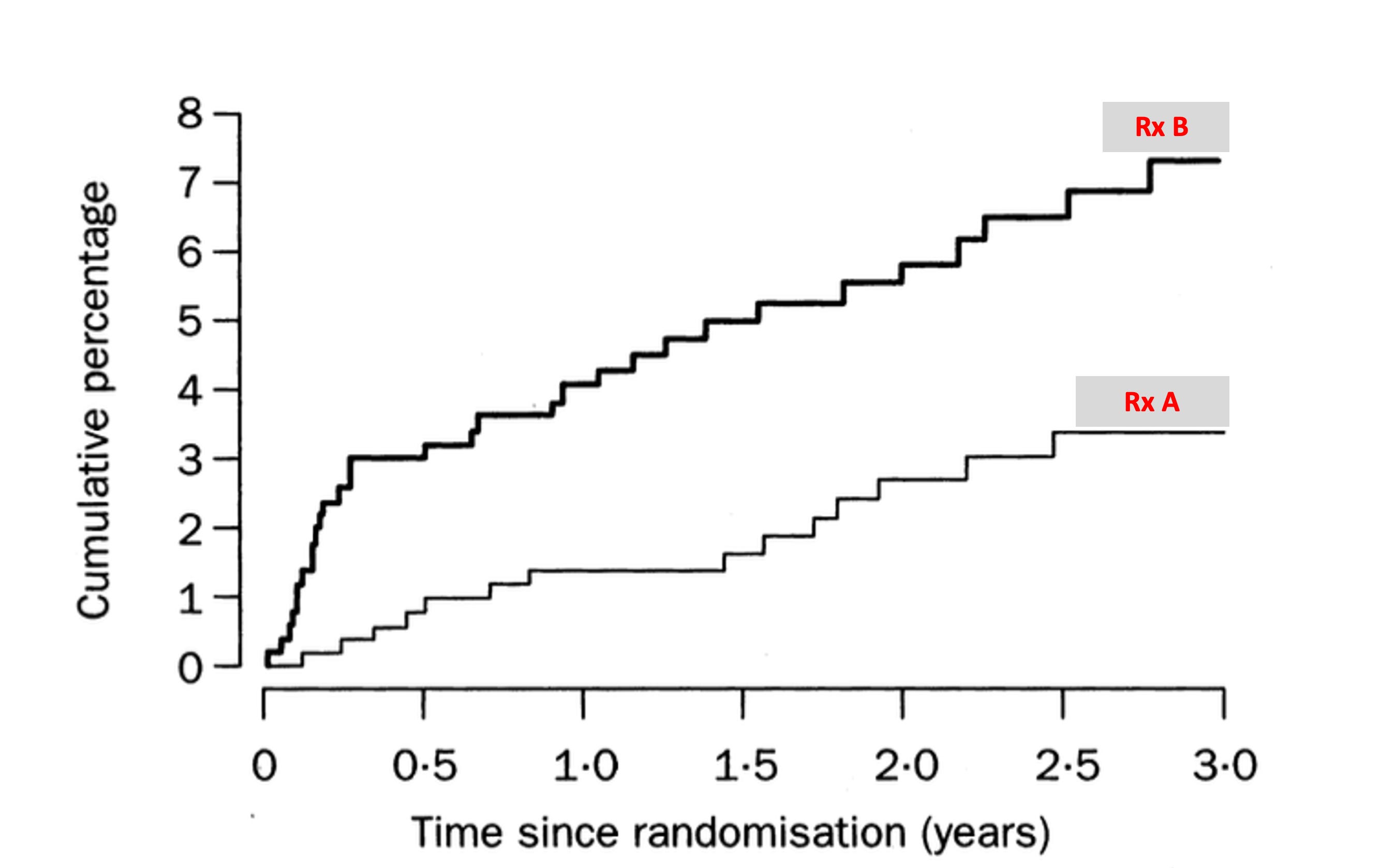
Which treatment would you want? Treatment A has a chance of dying or having a bad event of about 3%. Treatment B has nearly double the rate of these things.
It’s seems crazy to even ask. Of course the best treatment is treatment A. No one in their right mind would promote or volunteer to take Rx. B.
Ok. Now let me show you the specifics.
The Lancet published the Randomized Intervention Treatment of Angina (RITA-2) trial in 1997. It was done in 20 centers in the UK.

About 500 patients with coronary artery disease and a suitable lesion for angioplasty were randomized to medical therapy or angioplasty. (This was the early days of first generation stents; the majority of patients in the PTCA arm had plain old ballon angioplasty but some did receive stents).
The primary outcome was death or a myocardial infarction (MI). It should be noted that cardiac enzymes in 1997 were no where near as sensitive as they are now, so an MI in 1997 was often more substantial than MIs now.
Here was the actual KM curve of results.
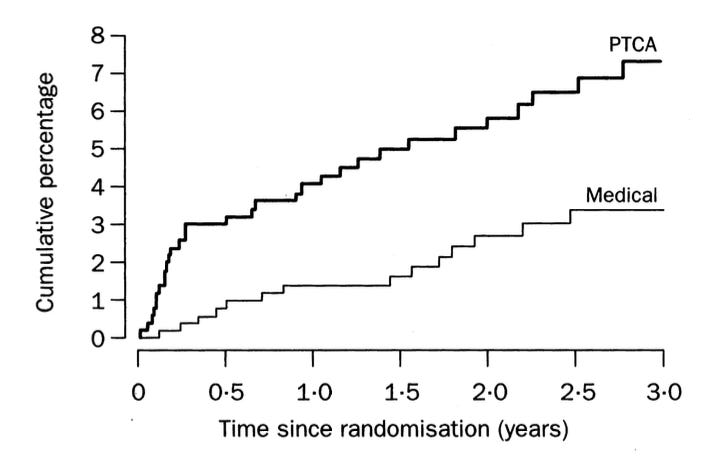
In written form: “Death or definite myocardial infarction occurred in 32 patients (6·3%) treated with PTCA and in 17 patients (3·3%) with medical care (absolute difference 3·0% [95% CI 0·4–5·7%], p=0·02).”
The authors also measured angina. Patients in the PTCA arm walked on average 35 seconds longer on a treadmill at 3 months. At 2 years, however, there were similar numbers of patients with grade 2 or worse angina.
Now I urge you to pause. Take a long slow cleansing breath.
I will copy and paste the authors’ conclusions. Keep in mind the basic tenets of medical science.
Interpretation In patients with coronary artery disease considered suitable for either PTCA or medical care, early intervention with PTCA was associated with greater symptomatic improvement, especially in patients with more severe angina. When managing individuals with angina, clinicians must balance these benefits against the small excess hazard associated with PTCA due to procedure-related complications.
Comments:
This study found a doubling of the hazard of the primary endpoint, death or serious heart attack.
The authors omitted that declaration in their conclusion. Instead, they called a 3 percent increase in death or heart attack a “small excess hazard.”
Spin is defined as language that distracts from an unfavorable primary endpoint. I can find no more egregious case of spin in the medical literature.
And to make matters worse, RITA-2 authors chose to emphasize a subjective endpoint, angina, in an unblinded study wherein one group received a major procedure and the other group had the blockage untreated except for tablets. What’s more, after 3 years, the rates of bad angina were similar in the groups.
You might argue, come on Mandrola, this was more than 20 years ago. It’s not relevant.
I would counter by saying that in the years following RITA-2, and the development of stents, there was a massive expansion of cardiology—not just the procedures to fix these stable partial blockages, but also the entire stress testing and imaging fields of cardiology to find the lesions. (The modern-day equivalent of stress imaging is coronary artery calcium scans—another express ticket to the cath lab and possible stents.)
I wonder about a counter-factual story wherein neutral scientists looked at curves like this and said—OMG. We are on the wrong tract with this percutaneous intervention approach. Medical therapy clearly looks better.
Then we may not have been surprised by the four trials—with null results—that I have just showed you in the last 4 weeks.
Instead of spending so much time and effort iterating better balloons and stents, we might have found better ways to treat the diffuse systemic disease of atherosclerosis.
As always, let me know what you think. We at Sensible Medicine have been stunned by your support. Thank you. We remain a user-supported site free of advertising.
Interesting thing about this is that because it's a hazard, not a benefit, the additional risk is described in absolute terms ("small additional risk").
Contrast to the way in which pharma products (think statins and mRNA covid injections) always describe their benefit using relative risk reduction.
I am sure that if the major event risk had been reduced from 3% to 1.5% instead of being increased from 3 to 6% the headline would have been "angioplasty halves risk of death or MI" not "angioplasty results in small reduction is risk of death or MI"
I agree this is dark stain on American medicine and it underscores the reason patients don't trust our system. Americans are subjected to these invasive procedures--you can count on that. But you can't count on receiving best practice medical therapy or optimal medical therapy (OMT) which is the most effective treatment for vascular disease. That is tragic, because if you compare OMT vs usual care in the same institution 10 times as many people die of cardiovascular and all causes after 4.5 years. Not 10%. 10 times. And you pay over $20,000 more per year for the privilege of increased risk. The American College of Cardiology now recommends OMT first but most people don't have access. It is past time to fix this. The problem is worse in women because the have heart attacks and die without chronic obstructive coronary disease. They are often told they have no heart disease.
https://pubmed.ncbi.nlm.nih.gov/20973686/