
If not for placebo procedures, you might be getting holes drilled into your heart
Two weeks ago, I wrote about how brave orthopedic surgeons saved many people from needless knee surgery. Yet cardiologists may be the bravest group of doctors when it comes to use of placebo trials

I started my private practice career in a place called Audubon hospital in Louisville Kentucky. For a medium sized hospital in a medium sized city, Audubon had a soaring history.
In 1984, 12 years before I walked in the doors, William J. Schroeder, age 52, had received the world’s second Jarvik 7 artificial heart. Though he soon suffered strokes, he lived nearly two years. Needless to say, the cardiac surgeons ran that hospital on the hill.
I soon learned of another cardiac surgical procedure that I had never heard of—transmyocardial revascularization or TMR. I had just finished training at Indiana University where I learned two new things in cardiology: percutaneous coronary intervention (stenting) and catheter ablation (then for SVT). But I had not once heard of TMR. At Audubon, TMR was done nearly every week.
Patients who had refractory angina due to severe coronary artery disease, which was not amenable to surgery or stents were referred for TMR.
Under general anesthesia, a surgeon made an incision in the side of the chest to expose the outside of the heart. The pericardium was opened and then tiny laser holes (1 mm) were drilled into the heart muscle, from the outside in.
In the 2 hour procedure, about 20-40 channels were made with the laser in the distribution where ischemia was felt to be most intense. The surgeon held pressure to stop any oozing. There was no need for going on pump. A TEE probe was used to prove that the laser holes had gone completely through the myocardium.
I remember consulting on these patients—as, with any cardiac surgery patient, they could develop rhythm issues. I asked: how does this work?
The plausible mechanisms were super interesting:
one was direct perfusion, which was borrowed from the reptilian heart where oxygenated LV blood could directly flow to the beating heart muscles.
Another mechanism was something called angiogenesis, where the laser injury triggered an inflammatory response and the heart would create new blood vessels that brought blood to ischemic myocardium.
A third way laser TMR might work is by denervating the heart muscle—rendering it incapable of sending pain signals.
I don’t remember any of the Audubon hospital believers tell me that such a technical procedure involving tiny lasers could work by placebo effect. But, indeed, placebo effect was surely possible.
What I do remember was people telling me: “John, I know it sounds crazy, but these patients feel better. They get less angina.”
TMR believers could even cite evidence. Numerous observational studies and even randomized trials had shown amazing results with laser TMR.
I made a slide of one of the typical studies, a Norwegian RCT published in JACC. In this test of TMR vs meds, angina was lessened in the TMR group.
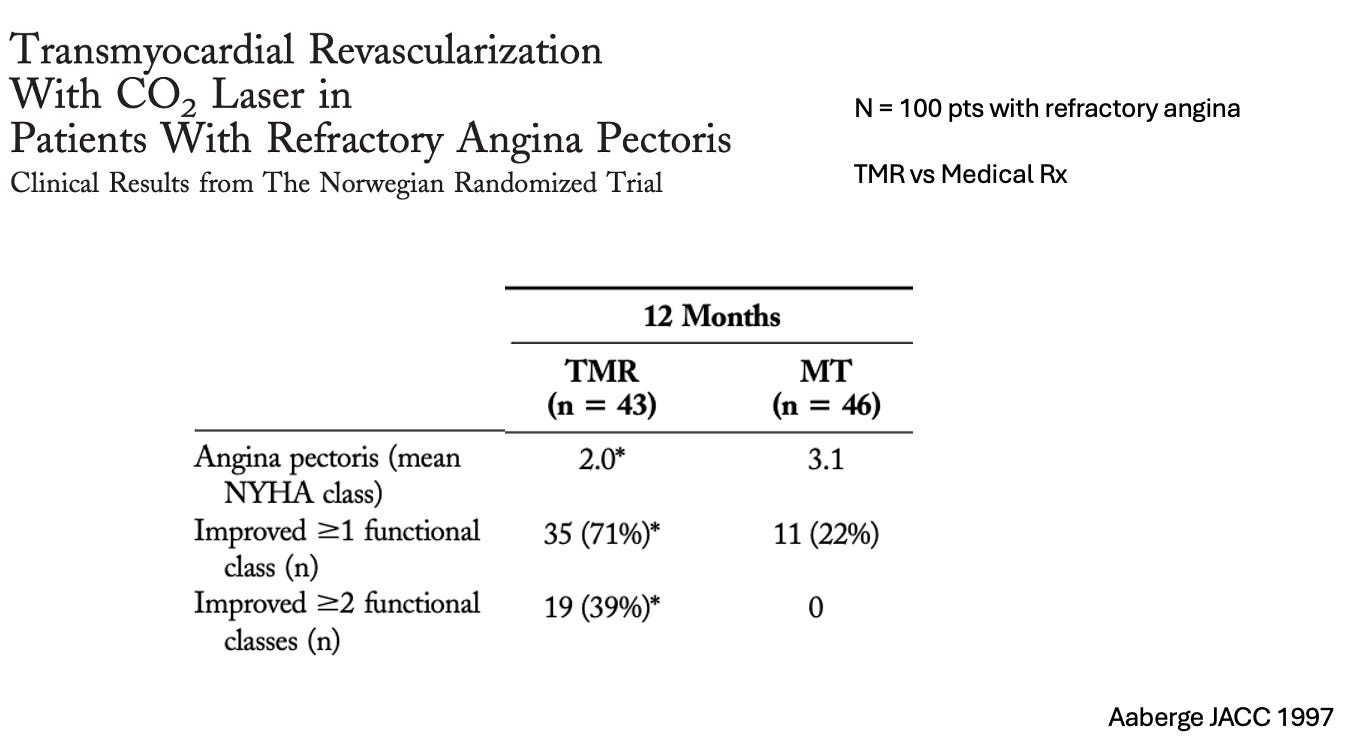
The problem with all these studies was either the lack of a control arm, or, in the Norwegian study, a lack of a placebo group.
TMR had received FDA approval in 1998, and rough estimates had over 20,000 TMR procedures performed in the US and over 50,000 worldwide.
As it happens with many surgical procedures, interventional cardiologists got involved and started doing percutaneous laser TMR, wherein a catheter was placed inside the LV and holes drilled from inside to out. It was the same concept—only without an incision in the left chest.
The Big Reversal Trial
In 2005, Dr. Martin Leon and colleagues finally got around to testing laser TMR in a placebo controlled trial. Nearly 300 patients with refractory angina were randomized to low-dose TMR, high-dose TMR or placebo (sham TMR). Their trial used percutaneous laser.
Every patient was heavily sedated, blindfolded and had earphones. The initial mapping part of the procedure was the same in all patients; after an acceptable LV map was obtained, wherein the doctors identified the location to place the holes, randomization was performed to one of the three groups.
It’s a beautiful protocol because it allowed preservation of blinding. Additionally, the the post-op care team was also blinded.
Here is a slide of the main results:
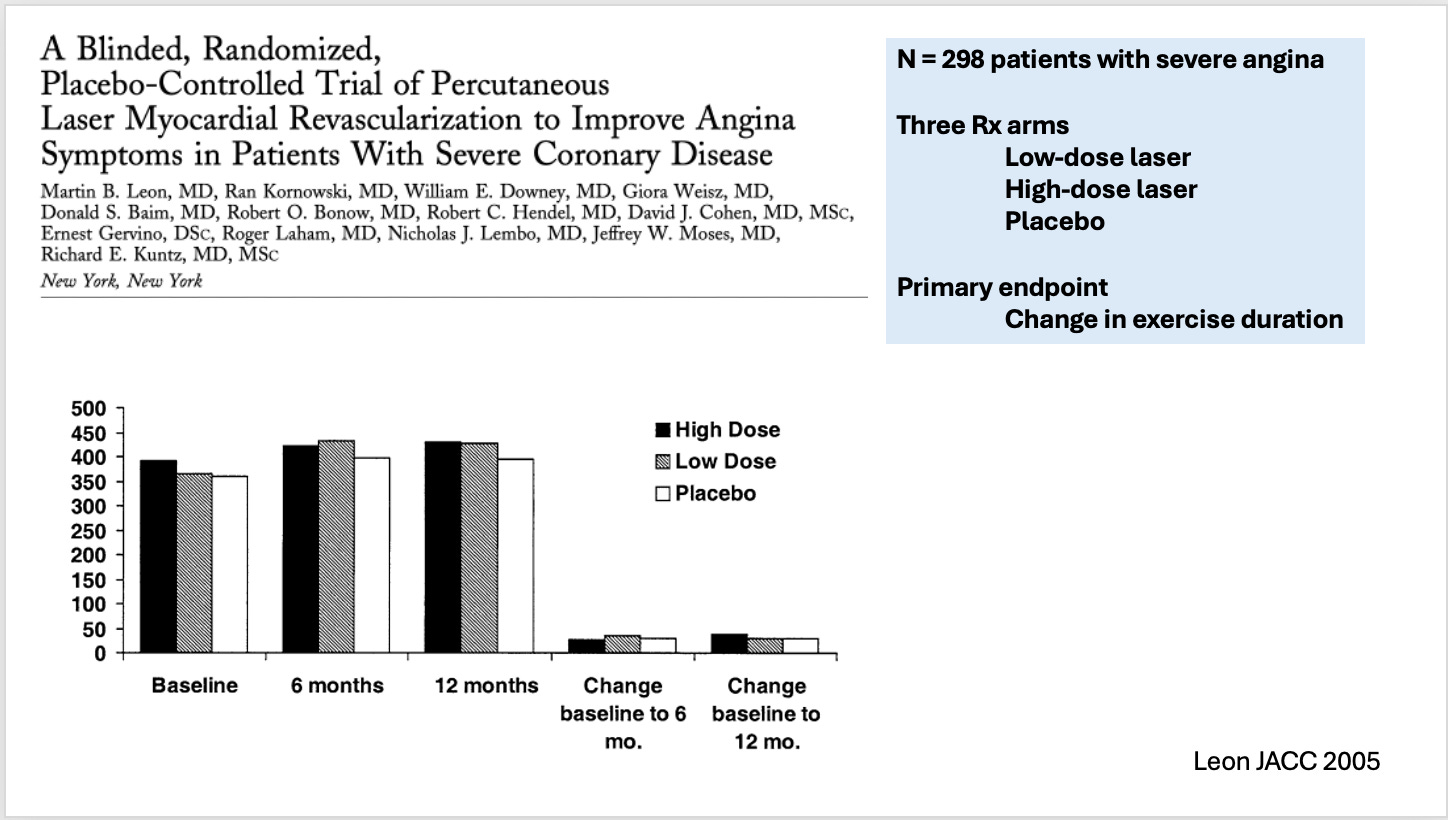
They found absolutely no difference in exercise time.
Interesting though was that all groups improved in angina symptoms—but the TMR group did not improve more than the placebo arm. Quality of life measures also did not differ among the groups. Tests for myocardial blood flow with radioisotopes did not differ.
Comments
I tell you this story because it again demonstrates the power of placebo control arms. It’s also notable because I lived through it, and remember smart people being cocksure that this procedure worked.
All of it undone by a group of doctors brave enough to randomize people to a placebo procedure.
Tens of thousands of patients were exposed to a highly invasive procedure that had no benefit. Cautious estimates of operative mortality were in the range of 5-9%, meaning nearly 1 in 10 patients died from a useless procedure.
TMR was established with a concoction of hubris, biologic plausibility and inadequate evidence.
The lessons from this story should be remembered whenever we recommend a procedure not tested with a proper sham control arm. Less than 300 patients randomized to a proper trial stopped a risky procedure done in tens of thousands of people.
Imagine a world, where we did such trials before exposing people to needless procedures. This should be a our goal going forward.
Thanks for the shout-out for what is still one of the most important and impactful trials that I've been involved in. One minor correction... the trial was actually enrolled between 1998-1999 and was scheduled for a LBCT presentation at TCT 2001, which was interrupted by the events on 9/11. After that, we got a little distracted for a while before the paper was finally written and published.
The childhood vaccine schedule has never been tested "with a proper sham control arm." Or even with a comparison of a vaccinated population vs an unvaccinated population.