
In Medicine, it's hard to challenge prevailing ideas
A small study challenged established thinking; the authors struggled to get their work published. The story of the AVATAR trial.

This one hits at the heart of my field—the ablation of atrial fibrillation.
Current thinking holds that the way to ablate AF is to electrically isolate the muscle bundles going in and out of the pulmonary veins. Think of it as building an electric fence around the pulmonary veins. We use different energy sources to ablate the tissue.
But one rule holds true. It is an absolute.
You must show that veins are electrically isolated after the ablation. Any leak of conduction, any tiny signal in and out of the vein is a failure. In fact, when we take patients back for a second procedure, it is usually to ablate gaps that have occurred around the veins.
Here’s the thing: it takes a fair amount of training, catheters, dollars, and skills to show the veins are completed isolated. When I do AF ablation, I show isolation using an expensive multipole catheter. It takes extra time. And you often have to be careful not to confuse signals from the left atrium as PV signals.
This rule keeps the ablation of AF within the domain of skilled electrophysiologists.
And that is why the AVATAR study had such trouble.

It looks like a pretty normal study in the picture. But it is not.
Here is why. The team from Imperial College London randomized about 300 patients with paroxysmal AF to one of three arms. One arm got AF drugs. Another arm got PV isolation using a cryoballoon, done in the standard way. Standard meaning the operators spent time checking to make sure the vein was isolated.
The third arm was the one that provoked my field. The third arm had cryoballoon ablation of the veins without checking the veins. They simply deployed the balloon, set the freeze time and did it twice. Then they got out of the left atrium. They called this the “Avatar protocol.”
Such a protocol is antithetical to standard EP. For decades, EP doctors take pride in our ability to show isolation of the veins. If you simply deploy a balloon and don’t measure anything, any doctor who works in the left atrium could do ablation of AF.
The “Avatar protocol” wasn’t the only curious thing about this study. Another novel part of the AVATAR trial was the choice of primary endpoint. Instead of measuring AF with a monitor, like most studies, the authors decided to measure what is most important to patients: time to any hospital episode related to treatment for atrial arrhythmia. IOW: did a patient require medical attention of an arrhythmia. (This, by the way, is exactly how private practice doctors, like myself measure AF ablation success.)
Here is what they found:
Both ablation arms crushed AF drugs. That was a given. Oodles of studies have shown this.
But here is the big slide:
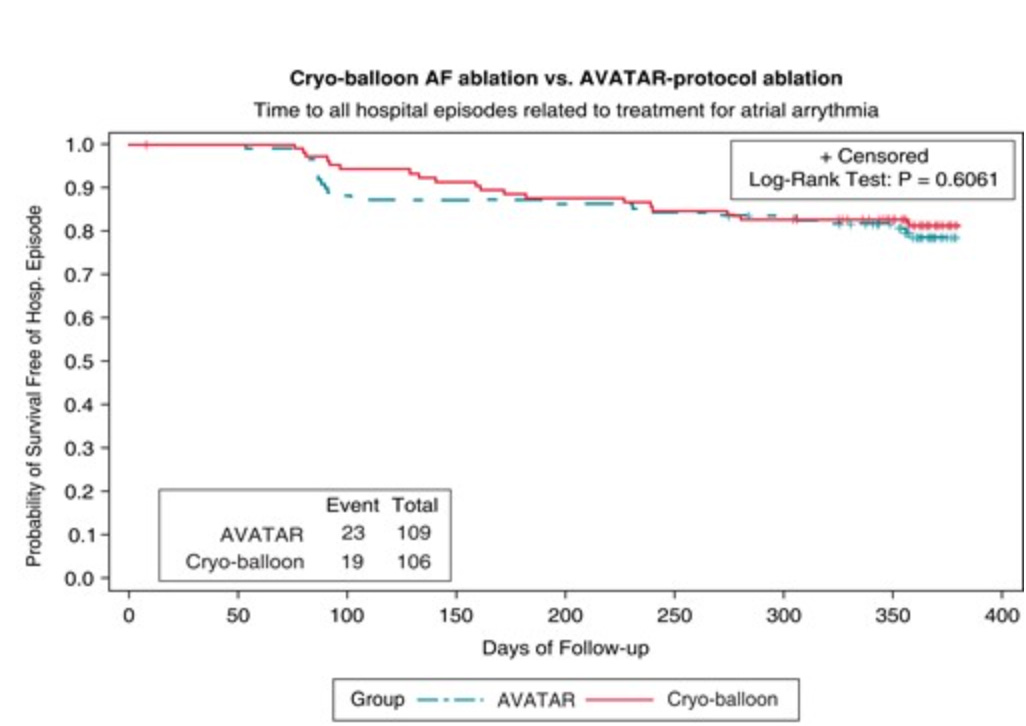
Boom. There was no difference in the two ablation arms. Simply deploying a balloon with no EP skills necessary produced the same result as a standard practice of carefully checking the veins.
The authors also measured quality of life. Every group, including the drug arm, improved, and there were no significant differences.
What about re-do ablation? You would think not checking for the quality of PV isolation would lead to more patients in the “Avatar arm” requiring redo ablation. Nope.
During the follow-up period, 9 patients (8%) in the AVATAR arm had a redo procedure following a primary endpoint compared to 15 patients (15%) in the conventional ablation arm.
The Struggle to Publish
The authors presented this data at the European Heart Rhythm Association meeting in 2019. Yet, you can see it was not in print until March 2023.

Here is another Tweet from an electrophysiologist.

Why was this so hard to publish?
Maybe you’ve detected the reason this novel finding did not make into the NEJM as a simultaneous publication? Instead it took nearly 4 years to publish in a smaller journal.
The reasons are…
a) it went against the current thinking, which disrupts the knowledge base of AF. We currently hold that PV potentials are core to the causation of paroxysmal AF, and must be totally eliminated. AVATAR authors show that you may or may not have to eliminate all the PV potentials.
b) is more important. The main reason this study had so much trouble is that it threatens the domain of electrophysiologists for AF ablation—one of our most lucrative procedures. If AVATAR is confirmed in a larger second study and we learn that AF ablation requires no EP knowledge, then that would be a serious problem.
Final Comment
I show this study because it makes you stop and think about the human aspects of medical science. The literature is replete with examples of provocative discoveries that had trouble gaining acceptance.
This one hits home. And I enjoyed telling you about it.
Sensible Medicine remains a reader supported endeavor. We have had a great year. Your support has been outstanding. Thank you. If you’d like to support us, here is the button:
Thomas Kuhn's ideas in action! Throw financial incentives into the mix, and it slows paradigm shifts even further. Now that docs like you are self-publishing, maybe you mavericks should all start your own non-profit journal for paradigm shifting research!
Unfortunately, this happens all the time in all fields of science, not just medicine. It's one of the reasons why I feel peer reviewed publications are obsolete vs open source journals with data transparency. The former seem to add no real value aside from acting as establishment gatekeepers.