
Initial Impressions of the LIBERATE-D Trial
This conservative vs standard approach to initiating dialysis for acute kidney injury is such an interesting trial, that I will introduce it today and discuss again in podcast form this Wednesday

When hospitalized patients become very ill, they may develop acute kidney injury. Many of these patients require dialysis to support them until (or if) kidney function recovers.
Examples of diseases that can injure the kidneys acutely include postoperative things, low blood pressure, kidney toxins, and sepsis.
The standard approach to dialysis is to put these patients on three-times weekly dialysis until they improve and can “fly” without support.
Some smart experts have proposed a conservative approach to dialysis, where it is deferred unless it has to be done. Reasons for this include super high levels of urea potassium, acid, fluid overload or this last nebulous one of clinical judgement.
JAMA published the LIBERATE-D trial.
Pause there and think about the study design. I like it. You are studying a new approach that exposes the patient to less aggressive care (because dialysis is quite aggressive) but you aren’t sure if it is better.
The conventional approach has been ensconced for years—without obvious trial support. Many readers of Sensible Medicine, including its founders are drawn to less-is-more strategies.
The primary endpoint of this experiment is kidney function recovery at discharge. The definition of “recovery” is being alive and not requiring dialysis for 14 consecutive days.
Two key secondary endpoints: number of dialysis sessions per week and the other was dialysis-free-days to day 28.
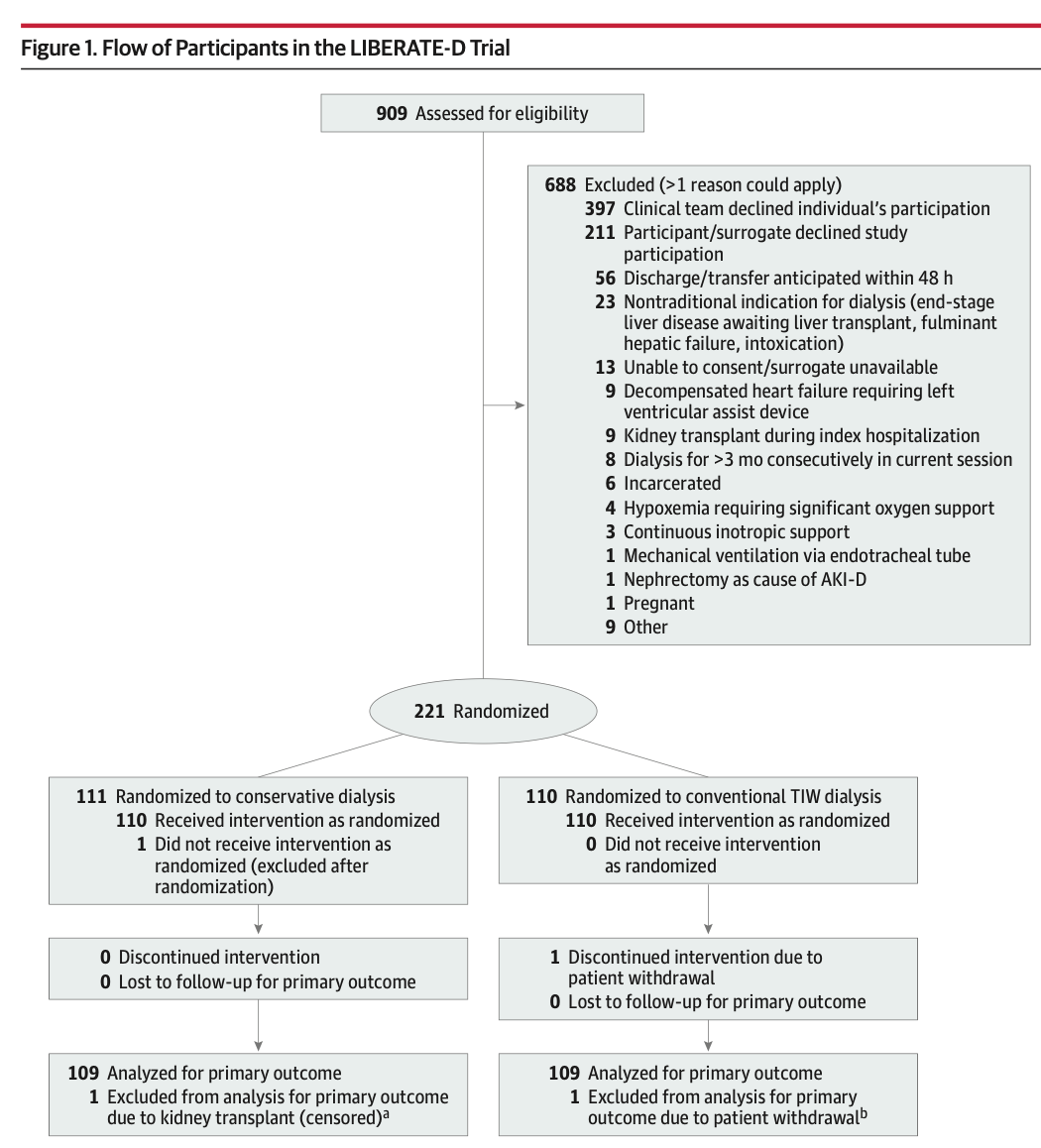
The flow diagram is copied below. You can see that they screened 909 patients to enroll only 221 patients. Most were excluded due to “clinical team declined their patient’s participation”.
The Main Results
The mean age of patients was young at 58 years. About 2/3rds were male, and 1/3rd had kidney failure from surgical procedures.
A primary endpoint of kidney function recovery at hospital discharge occurred in 64.2% of patients in the conservative arm vs 50.5% in the conventional three-times weekly dialysis arm. The estimated difference of 13.8 had 95% CI of 0.8-26.8) and a p-value of 0.04.
The authors also provided relative risk results. Here the unadjusted odds ratio was 1.76 (95% CI 1.02-3.03; p = 0.04). However, in the statistical plan, they set out that they would do an adjustment based on baseline variables.
In the adjusted analysis the odds ratio decreased to 1.56 and the 95% CI now included the lower bound less than 1 at 0.86-2.84; p =0.15).
The two key secondary endpoints all favored the conservative approach. Dialysis days were 1.8 vs 3.1 and dialysis-free days was 21 vs 5 in the conservative vs standard approach. I find these curious endpoints because—by definition—a conservative approach will have fewer dialysis sessions. That is the strategy.
Another important endpoint was that the time to kidney function was faster in the conservative arm: 2 days in the conservative dialysis group and 8.5 days in the conventional dialysis group.
There were no other differences in major outcomes such as in hospital death.
Comments and Questions
We like this trial because the authors are trying to answer a common and important clinical question. This differs from many studies which are designed to sell a drug a device. In the science vs marketing category, this is science. Good.
The second question is study design. The authors designed it as superiority test. They assumed that the conservative approach would be 20% better than the conventional arm. That seems aggressive. My question here is why did they not choose a non-inferior test in that the conservative arm is less invasive, less costly and less burdensome. You’d mainly want to show that it was not substantially worse.
A corollary question now arises is whether you can interpret these results where the conservative arm is 56% better as non-inferior. I mean the lower bound of that odds ratio went to 0.86, meaning that it could be 14% worse. Would that fall within a non-inferiority window? I am asking.
The third question is whether we should hue to the formal statistical interpretation that there was no statistical difference between the two strategies given that the adjusted results had a p-value of 0.15.
I ask, because clearly the conservative arm led to 14% greater rate of kidney recovery. If we did a Bayesian conversion of these results, I suspect the Pb of any benefit would be very high.
This third question is crucial for clinical decision making: to wit, there were fewer dialysis days in the conservative arm, no substantial adverse effects, and a strong trend to better outcomes. No, the results did not reach the statistical threshold, but does not mean they should be discounted?
The fourth question relates to the selection of patients. The authors screened 900 to enroll 200. So this was a select group; a group that the clinical teams felt were well enough to be studied. The vast majority of screen failures were by the clinical teams rejecting trial inclusion. Why? Is equipoise in question?
The authors were very clear about these limitations and cautious about not making strong conclusions. They called for a larger trial to try to sort out the uncertainty inherent in the wide confidence intervals.
The question remains: when you have a patient like one in the LIBERATE trial, is this data enough to pursue a conservative dialysis strategy?
Tune in to our Fortnight podcast Wednesday and hear the view of Adam and Andrew—two of the best thinkers on evidence in the medical field.
I think this study gives comfort to those who dialyze only when it is absolutely necessary to prevent life threatening complications, like the AEIOU I learned in training.
I’m confused by this study. When I was an IM resident (late in the last century), on in-pt renal rotation we offered RRT for pts with persistent hyperkalemia, acidemia, and/or volume overload refractory to med Rx, or uremic symptoms. The “conservative strategy” was THE ONLY strategy at the time. When I’m on CCU now, I consult Nephro for IHD for those same reasons. And our nephrologists only offer it for those indications. What exactly is the “standard of care” in those 4 hospitals? Are they dialysing people just for a serum Cr number? If so, that seems insane.
I agree a “non-inferiority” design would have been more appropriate. Less invasive, less cost….”not worse” would have been plenty good enough to adopt this over the “conventional” standard.