
Is One of the Most Popular Cardiac Drugs Better than its Generic Competitor?
The British Medical Journal has reignited a 14-year debate regarding the antiplatelet drug ticagrelor (Brilianta) and PLATO trial

When you read the PLATO trial in the NEJM, nothing seems awry.
It was a comparison of ticagrelor vs clopidogrel as the second antiplatelet drug (added to aspirin) in more than 18,000 patients who were having an acute coronary syndrome (most often an MI).

The primary endpoint of CV death, MI or stroke occurred in 9.8% in the ticagrelor arm vs 11.7% of those on clopidogrel. The HR was 0.84 with 95% confidence limits ranging form 0.77-0.92 and a P-value equal < 0.001. This is a clinically meaningful and statistically robust finding.
Ticagrelor is a more potent antiplatelet drug than clopidogrel (and it works differently), but major bleeding was not significantly different.
Yet ticagrelor did not pass muster during its first pass at FDA. Underneath the surface of these top line findings was oodles of controversy.
Over at Cardiology Trials Substack, a project to chronicle all of cardiology’s seminal trials that I co-author with Andrew Foy and Mohammad Ruzieh, the first time we covered PLATO, we failed to note the massive controversy—because it was not obvious from the NEJM publication.
We published this revision today.
The Massive Stakes of Being Wrong about Ticagrelor
Coronary stents have been an amazing intervention for patients having acute coronary events, but a downside is that antiplatelet drugs are required to keep the stent from clotting off the vessel.
The most common antiplatelet is generic clopidogrel (Plavix). A potential problem with clopidogrel is its complex metabolism wherein a non-small number of people do not get the full antiplatelet effect. Despite these issues, clopidogrel has held up well in clinical trials and remains the most common antiplatelet drug in addition to aspirin after coronary stenting.
Ticagrelor is an expensive blocker of platelet function, used often after a complex percutaneous coronary intervention (PCI). In 2022, the US federal government spent more than $750m on ticagrelor. That’s just one year; it’s been approved for more than decade. For instance, despite being only 7% of the antiplatelet market in 2020, ticagrelor accounted for nearly two-thirds of medicare spending on antiplatelet drugs in 2020.
There is another antiplatelet drug on the market. Prasugrel is also a more potent antiplatelet and it is taken once daily vs ticagrelor’s twice daily dosing. Despite prasugrel crushing ticagrelor in the ISAR-REACT 5 trial, ticagrelor remains the favored drug when doctors feel they need more than clopidogrel.

The PLATO Controversy
Foy, Ruzieh and I have revised our PLATO coverage over at CardiologyTrials. The BMJ investigation is here but is paywalled.
Here is a list of problems.
1 Mortality Benefit Questioned
Shortly after PLATO was published, Drs. Victor Serebruany and Dan Atar wrote an editorial in the European Heart Journal titled: The PLATO trial: do you believe in magic?
Ticagrelor reduced overall death by 22%. This was larger than the MI and CV death reduction. Bleeding rates were numerically higher in the ticagrelor arm. The question was how can the drug reduce death if not by reducing cardiac events or bleeding.
Maybe it was the play of chance. But maybe not. The BMJ investigation also noted concerns about the accuracy of death records. Here is a screenshot of what we quoted from the BMJ.

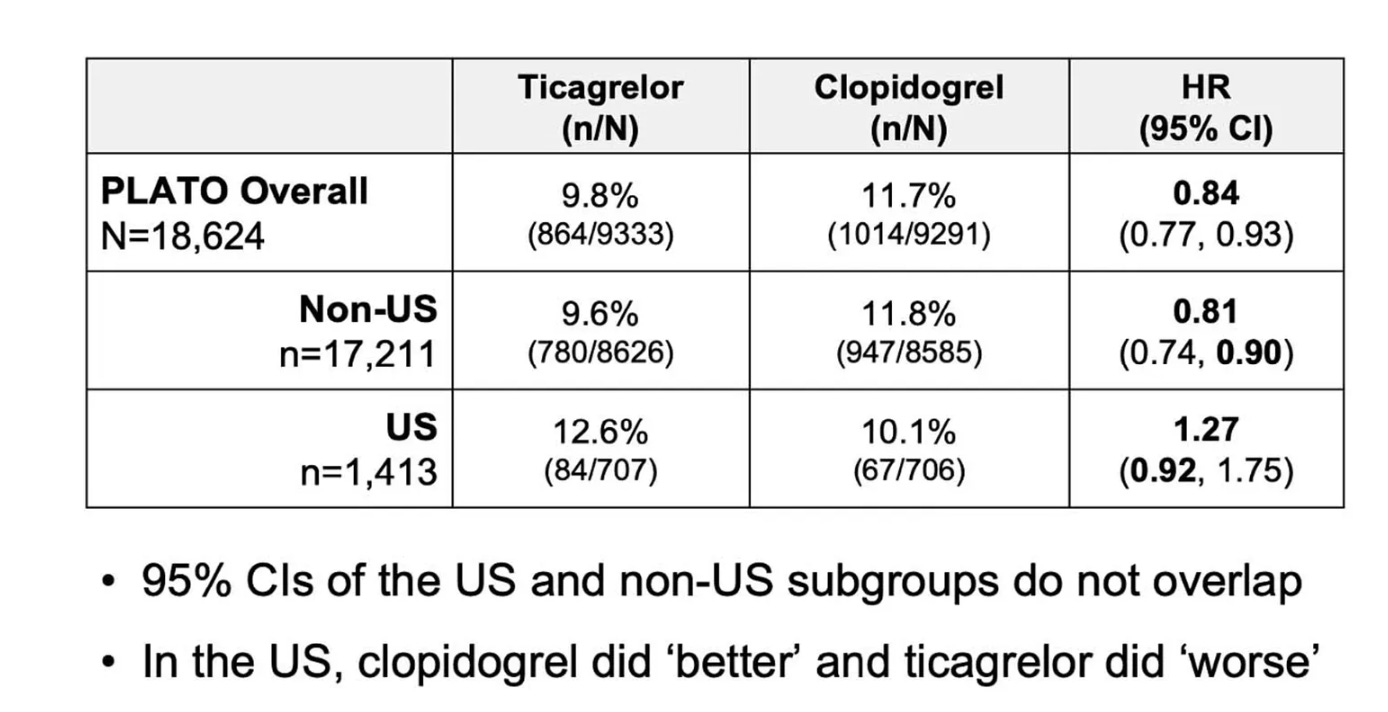
2 Unexplained Regional Variation of Effect
Below is a slide from the FDA. In the US, clopidogrel did much better than ticagrelor. Why would ticagrelor be 27% worse than clopidogrel in the US when it was 16% better every where else?
FDA was very concerned about this. The advisory committee at FDA recommended that the company run another trial. FDA disagreed and asked the company to resubmit the drug with further analysis to explain why ticagrelor underperformed in the US.
Proponents of ticagrelor might say, John, it is a subgroup. It’s underpowered and if you look at enough subgroups, it might just be the play of chance—like the famous astrological effect on post-MI aspirin seen in ISIS-2. This is the problem with subgroups. It’s hard to know.
The PLATO authors offered another explanation: US patients often took higher doses of aspirin. Whereas most of the world was using low-dose aspirin as part of the dual antiplatelet regimen, the US used higher doses. In our PLATO revision piece, we cite a complicated statistical analysis supporting the theory that aspirin dose caused the geographic variation. Foy, Ruzieh and I struggle to understand how ASA could do this, given the fact that major bleeding was not different in the US.
Now it is time to sit down. Slow down your reading. Because there is another potential cause of this variation. And it is not easy to write about.
It turns out that most of countries and sites were overseen by the company. Four countries, however, were overseen by a neutral contract research organization or CRO. US sites were overseen by a CRO, not the sponsor. In fact, of the four countries supervised by CROs, US, Israel, Russia and Georgia, all had numerically higher rates of events in the ticagrelor group.
That could just be chance. But let me tell you something else.
3 Concerns Regarding Event Adjudication
As detailed in the BMJ investigation the site records indicated 504 MIs in the ticagrelor group vs 548 in the clopidogrel group. Most trials have a central adjudication committee which confirms or refutes or adds to these numbers.
In PLATO, after adjudication, the count increased only for the clopidogrel group, reaching 593. That is 45 more MIs in the clopidogrel group vs 0 in the ticagrelor group. I leave that with no comment.
4 Lack of Replication of Ticagrelor superiority over Clopidogrel
PLATO was published in 2009. There has been ample time for other evidence to support its strong finding of ticagrelor superiority over clopidogrel.
But neither any observational study nor two RCTs have found ticagrelor superiority over clopidogrel. And I have already told you how badly ticagrelor failed against prasugrel in ISAR-REACT 5.
This is curious. Most cardiac drugs these days, such as ACE-I, beta-blockers, mineralocorticoid antagonists, SGLT2i, and GLP1a all look positive in multiple trials. The exception of course is sacubitril/valsartan.
To be fair to the PLATO investigators, they have responded to these criticisms in multiple pieces. Here are links to four of their rebuttals.
Thrombosis and Hemostasis https://www.wellesu.com/10.1160/TH11-03-0162
Stroke https://www.ahajournals.org/doi/10.1161/strokeaha.111.000514
Inter J of Cardiol https://doi.org/10.1016/j.ijcard.2014.06.029
Circulation https://doi.org/10.1161/CIRCULATIONAHA.111.047498
Conclusion
I encourage you to read the BMJ paper and our revised view of PLATO. The public documents from FDA are also available. As our the authors’ replies.
Note also that the DOJ started an investigation but concluded it after about a year, saying, “that the allegations lacked sufficient merit such that it was not in the best interests of the US to intervene in the suit.”
I stand with the FDA advisory committee in recommending a confirmatory trial. This was not done, and likely will not be done, 14 years later.
But imagine if ticagrelor was not more effective than basic clopidogrel.
I don’t prescribe antiplatelet drugs, but as an appraiser of evidence, it’s hard to read these issues and have confidence in ticagrelor superiority over clopidogrel.
Comments are welcome. Tell me what I am missing. Tell my why we shouldn’t have two confirmatory trials or a mandated post-approval trial with new drugs that will have common indications. JMM
If you appreciate this content, please consider becoming a free or paid subscriber. Sensible Medicine remains an industry-free source of medical content.
You are right. The whole “aspirin dose” hypothesis is silly. They pulled that excuse literally right out of their arse. PLATO used mainly 300mg load plavix, whereas most docs use 600mg. The drug eluting stents during that trial were older versions (ie higher thrombosis rates; not applicable to today). I recall being in several conference discussions during that time when heated debates would arise about PLATO limitations/critiques and anytime somebody questioned the results, the answer was to essentially squash any further discussion. I recall getting the sense that nobody really wanted to seriously debate the merits of this trial and they are looking to just get another patented drug approved. Soon after, lots of emergency rooms, chest pain units, ICUs, in the adopted “Brilinta” as the drug of choice for acute coronary syndrome. The side effect of dyspnea was obviously understated in the study. The actual incidence of dyspnea as a result of this drug is much higher and I have had to discontinue it in multiple patients. Patients are always complaining about the out-of-pocket cost. The whole clopidogrel non-responder issue, while real, was highly exaggerated.
So yes, absolutely it’s time to revisit this medication. Will it happen? Doubt it.
PLATO was a scam.
The standard dose of Clopidogrel loading in ACS is 600 mg.
In PLATO, Ticagrelor was tested against only 300 mg of Clopidogrel.
substandard and under-dosing of the control arm explains the apparent superiority of Ticagrelor.