
Is Shortness of Breath Due to Heart Failure Different from Shortness of Breath Due to Asthma?
Another favorite article

There are articles that change your practice. There are articles that clarify your understanding of medicine. There are articles that are great examples of study types, bias, and design errors. And then there are the articles that are just so interesting that although they don’t really impact the medicine you practice you find yourself referencing them every few months.
I have always liked it when people describe parts of the body as inarticulate. The brain is articulate as injury to it produces diverse, diagnostic symptoms – encephalitis speaks differently than a brain tumor speaks differently than a right MCA stroke. The lungs are less articulate; pulmonary diseases can only say shortness of breath and a dry cough.
Separately, our language is just not up to describing some symptoms.[i] If someone complains of pain, we immediately work to have people better articulate what they are feeling. Is it burning, or tingling, or aching, sharp or dull, lancinating? When people complain of shortness of breath, we mostly respond with “oh.” (And then we’ll write in the chart that they are dyspneic). We’ll ask some version of the PQRST (What are the palliative and provocative features, what is the quality, does it radiate, what is the severity, what is the timing). But we don’t go any further in determining what the dyspnea feels like. Why? It is because we think all dyspnea feels the same and thus trying to define the sensation has no diagnostic value.
That is where the article Descriptors of Breathlessness in Cardiorespiratory Diseases comes in. The study was a pretty simple one. The researchers had two goals, to assess the reliability of descriptors of dyspnea – did patients describe their dyspnea the same way over time and could they recall what their dyspnea felt like? – and to assess if different diseases were associated with different descriptors.
The authors recruited patients who had been referred for pulmonary function testing and answered yes to the question, “Do you have 'uncomfortable awareness of breathing' with activities?" PFT findings and clinical histories were used to diagnosis patients and those included had one of 7 diagnoses.[ii] The patients were then asked to choose descriptors of their dyspnea from a list of 15:
1. My breath does not go in all the way.
2. My breathing requires effort.
3. I feel that I am smothering.
4. I feel hunger for air.
5. My breathing is heavy.
6. I feel out of breath.
7. My chest feels tight.
8. My breathing requires work.
9. I feel that I am suffocating.
10. My chest is constricted.
11. I feel that my breathing is rapid.
12. My breathing is shallow.
13. I feel that I am breathing more.
14. I cannot get enough air.
15. My breath does not go out all the way.
These questions were grouped into 10 clusters which the researchers called the work/effort cluster; suffocating; exhalation; tight; inhalation; shallow; rapid; breathing more; heavy; air hunger.
Among the results, the authors provide data about the most common ways that people with the various illnesses described their dyspnea. (Table 5) Patients with any of the conditions used the descriptors in the cluster work/effort. Patients with COPD only used these descriptors. Other diagnoses had more distinct distributions of descriptors.
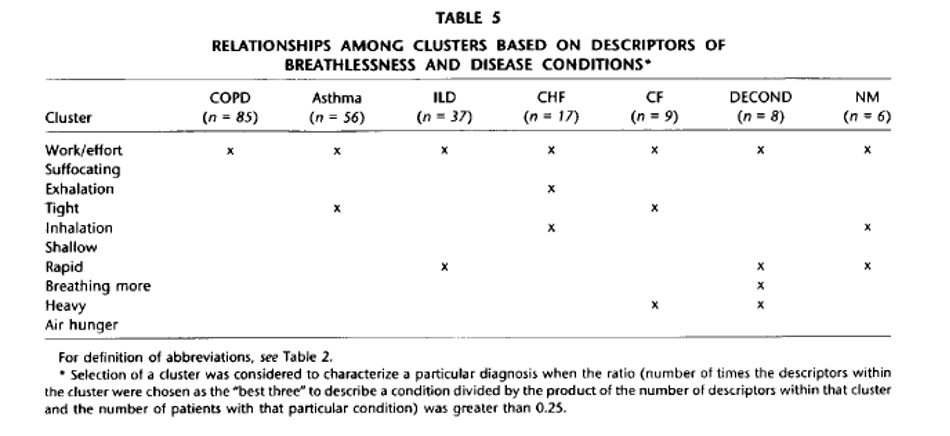
As you can tell from this table, there was too much overlap of the clusters (or the individual descriptors) to make them useful diagnostically. There is not a magic descriptor that if used by a patient means she has asthma. (One interesting point: The authors stayed away from making any claims, nor did they present test characteristics, but from the table it seemed that the descriptor “my breath does not go out all the way” had a sensitivity and specificity for HF of 29% and 100%.)
Why is this clinically useless paper one of my favorites? I think it hints at the complexity of a symptom that I encounter nearly every day. I leave the article feeling like a person in an asthma exacerbation is experiencing different shortness of breath from a person with pulmonary edema. Maybe, if we grew up in a world where we all experienced all the causes of dyspnea from an early age, our language would have evolved to have different words for every flavor of dyspnea. It would be a terrible world, but the diagnosis of dyspnea would be a whole lot easier.
[i] I so desperately tried to stop myself from making reference to the Inuit and all their words for snow. I managed to keep it out of the body but not the footnotes. Here are just a few of the words:
qanuk: 'snowflake'
kaneq: 'frost'
kanevvluk: 'fine snow'
qanikcaq: 'snow on ground'
muruaneq: 'soft deep snow'
nutaryuk: 'fresh snow'
pirta: 'blizzard'
qengaruk: 'snow bank'
[ii] The 7 diagnoses were COPD, Asthma, ILD, CHF, cystic fibrosis, deconditioning, or neuromuscular disease.
I think I’d get myself into too much trouble joking about the “shortness of breast” typo so I’ll just say thanks for a great post! : )
As per usual, Dr. Cifu’s article is enlightening, thought-provoking, and insightful.
Although my comment is not directly related to the content of the article, there is one pearl that has served me well in differentiating “shortness of breath“ in emergency situations.
The tachypnea of hyperventilation versus acidosis: In hyperventilation, the stimulus is neurobiological, and the emphasis is virtually always on inspiration. In the acidotic patient the emphasis is on expiration in an attempt to blow off as much CO2 as possible in an attempt to correct the acidosis. The diagnosis of DKA in the diabetic patient can often be made at the bedside, even before the glucose and pH is determined.
Ben Hourani MD