
Nirmatrelvir for Vaccinated or Unvaccinated Adult Outpatients with Covid-19
It's mid 2026 and NEJM publishes another decidedly negative Paxlovid trial. A couple of lessons emerge: one about evidence expiration dates and the other about incentives to delay trial publication

I almost missed the trial. Hidden amongst the cardiology, oncology and ICU trials in the New England Journal of Medicine, was a relic from the time many of us try to forget—the pandemic.
This is a story about how changing disease environments can change drug efficacy. And why trials need to be repeated when times change.
During the early parts of the pandemic, before vaccination and before enough people had been exposed to the SARS-CoV-2 virus, a trial called EPIC HR found that treatment of symptomatic Covid-19 with nirmatrelvir plus ritonavir (Paxlovid) resulted in a risk of progression to severe Covid-19 that was 89% lower than the risk with placebo. This highly positive trial led to strong recommendations to use this medicine in such patients—despite the large number of potential drug-drug interactions.
The pandemic then changed. People were vaccinated; others were infected and developed immune protection to the virus. The next question became: would the antiviral medication have the same effect in vaccinated or previously infected individuals.
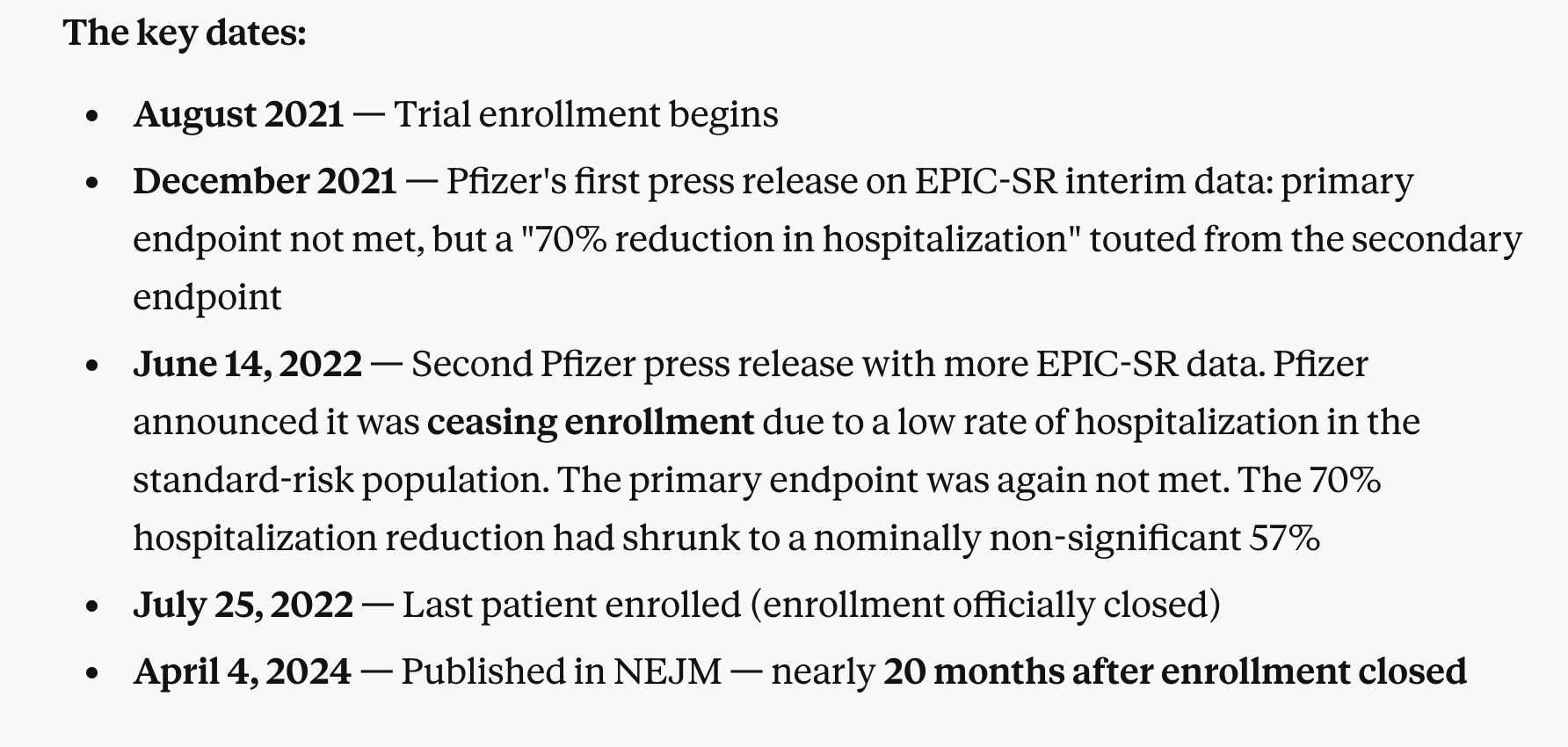
The EPIC-SR (standard risk) trial, published in 2024, randomized 1296 patients to placebo or nirmatrelvir–ritonavir and found no difference in the primary endpoint of time to sustained alleviation of all COVID-19 symptoms. A cursory look at this seems anodyne. Patients were low-risk; the drug therefore had no significant effect.
But the timeline is bothersome. I asked CLAUDE for some help sorting this out.
The Current Paper (April 2026)
The NEJM manuscript published last week included results of the British PANORAMIC and Canadian CanTreatCOVID trials. Both enrolled higher risk older patients with a coexisting condition who tested positive for SARS-CoV-2 and had been unwell for 5 days or less.
The randomization was to usual care plus nirmatrelvir (300 mg)–ritonavir (100 mg) twice a day for 5 days or to receive usual care alone. The primary outcome was hospitalization or death from any cause within 28 days after randomization.
Enrollment was carried on between Sept 2021 and Sept 2024.
In the PANORAMIC trial, 14 of 1698 participants (0.8%) in the nirmatrelvir–ritonavir group and 11 of 1673 participants (0.7%) in the usual-care group were hospitalized or died. Clearly not a significant difference. In the CanTreatCOVID trial, 2 of 343 participants (0.6%) in the nirmatrelvir–ritonavir group and 4 of 324 participants (1.2%) in the usual-care group were hospitalized or died.
Serious adverse events with nirmatrelvir–ritonavir were reported in 9 participants in the PANORAMIC trial and in 4 participants in the CanTreatCOVID trial.
One secondary finding of note: Symptom recovery was faster with nirmatrelvir–ritonavir. Median time to recovery was 14 days vs. 21 days in PANORAMIC, and 6 vs. 9 days in CanTreatCOVID. The problem, of course, was that these were pragmatic open-label trials without a placebo, and symptom recovery is subjective and susceptible to placebo and nocebo effects.
The authors concluded:
In two open-label trials, nirmatrelvir–ritonavir did not reduce the incidence of hospitalization or death among vaccinated higher-risk participants with SARS-CoV-2 infection.
Comments
Keep reading with a 7-day free trial
Subscribe to Sensible Medicine to keep reading this post and get 7 days of free access to the full post archives.