
Nirsevimab (Beyfortus): is universal prophylaxis for RSV warranted?

Dharini Bhammar, PhD, MBBS, is a respiratory physiologist and evidence enthusiast. As a new mum, her pediatrician recommended the RSV monoclonal antibody for her baby. After reviewing the evidence, she declined it. We are excited to share her clearly written argument as an excellent example of evidence translation. Core concepts discussed include effect size, net benefit and the external validity of clinical trials. I wish more clinicians thought like this. JMM
As a new parent, I was offered Nirsevimab for respiratory syncytial virus (RSV) prophylaxis for my healthy term infant in October (when she was 3 months of age). Nirsevimab is a human recombinant monoclonal antibody with activity against RSV that is sold under the brand name Beyfortus. It is now recommended by the CDC and by European countries for all babies < 8 months from Oct-Mar (RSV season) with some caveats such as maternal RSV vaccination status. The purpose of universal prophylaxis is to reduce RSV-associated hospitalizations.
For RSV-associated lower respiratory tract infection (LRTI) hospitalizations, three studies found a significant effect and two found a null effect. Note the immunization efficacy estimate[i] crossing zero for Hammitt and Simoes in the truncated table from a 2024 meta-analysis by Ricco et al.

Two of these studies, Hammitt and Drysdale, included healthy term infants. Hammitt et al. (N=1490), the MELODY trial, showed a small decrease in the primary endpoint of medically attended RSV-associated lower respiratory tract infection through 150 days post injection (primary end point of the study). The figure (after removing the inset that magnified the small effect) is below.

The secondary endpoint of hospitalization for RSV-associated LRTI occurred in 0.6% patients in the Nirsevimab group vs 1.5% in the placebo group, respectively. (P=0.07). Supplemental table S6 shows that average days hospitalized for RSV-associated LRTI in the Nirsevimab group is 7.2 and placebo group is 4. The FDA briefing document includes a figure with relative risk reductions plotted for term infants, with wide confidence intervals for RSV hospitalizations.

LRTI from any cause was not significantly reduced (2.3% for Nirsevimab, 4.1% for placebo; 95% CI for efficacy -15.8 to 71.7). Number needed to treat (NNT) to prevent hospitalization from RSV ranged from 32 to 223 and for LRTI from any cause 31 to 500.
Drysdale et al (the HARMONIE trial conducted in Germany, France and the UK) was an open label RCT in healthy infants <=12 months of age. RSV hospitalizations were significantly reduced (11 out of 4037 in Nirsevimab group vs 60 out of 4021 in the standard of care group; see figure below).

Very severe RSV was also reduced (5 out of 4037 in Nirsevimab group vs 19 out of 4021 in the standard of care group).

Hospitalization for LRTI from any cause (an important outcome) during the RSV season occurred in 45 infants in the Nirsevimab group and in 98 in the standard-care group (also statistically significant but with marginal efficacy of 58% percent). Subgroup analysis demonstrated a possible heterogenous treatment effect with most of the benefit isolated to infants less than 3 months old.
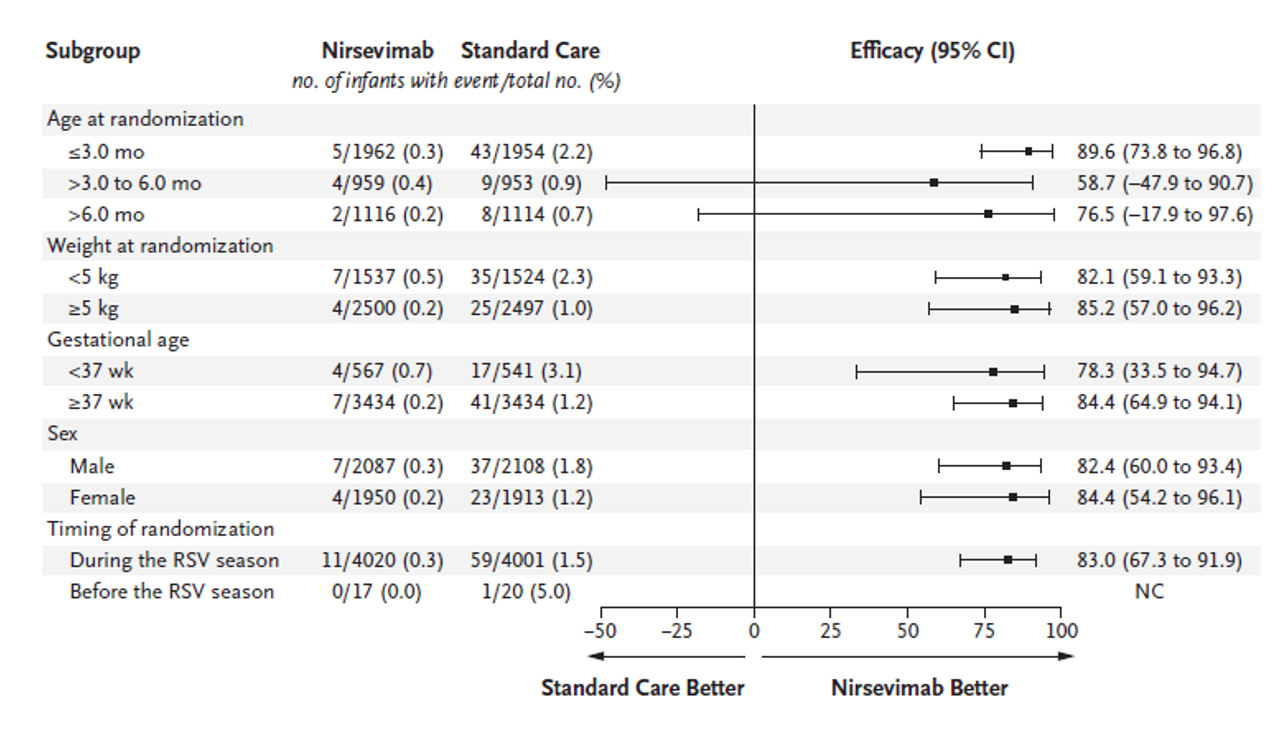
The NNT from Drysdale is 77. Data are not available for all cause hospitalization by term/preterm status. But for RSV hospitalization, NNT is 100 for term infants.
Medical decision making always includes safety signals. From Drysdale, serious events were 2.2% in Nirsevimab group and 1.7% in standard of care group. This gives a number needed to harm (NNH) of 200. No deaths were reported in either group. It should be noted that mortality is almost unheard of for RSV infections in developed countries.
The FDA adverse event reporting system (FAERS) has reported 280 events (14 deaths) after Nirsevimab in 2024 (260 of these were reported by a healthcare professional). The breakdown of causes: 44% were “drug ineffective", 31% were RSV bronchiolitis, 22.5% bronchiolitis. In my opinion, 14 deaths seems excessive and something that should be further explored.
The RESCEU birth cohort study showed that most hospitalizations for RSV are before 3 months of age (0.97%). After 3 months, the risk is <0.5%. There are known risk factors for RSV hospitalization: attending daycare, older siblings with symptomatic RSV, underlying disease, preterm, secondhand smoke exposure. Breastfeeding for 4-6 months is associated with a protective effect on RSV hospitalization.
The cost of Nirsevimab is about 50 euros per dose in Europe. The cost in the US (Xpress Scripts) is $1350-1450 per dose (fully covered by my insurance). At 3.6 million babies born per year in the US, that amounts to $4.8 billion/year.
You also can’t read a single paper on this topic without noticing the long list of conflicts of interest for study authors.
A summary of weaknesses in the studies:
1. RCTs with healthy term infants still included preterm infants. Why not complete studies in only healthy term infants?
2. No a priori consideration of breastfeeding in any study. Breastfeeding is likely to be a strong effect modifier. No consideration of other known effect modifiers.
3. Substandard primary outcomes like medically attended RSV in lieu of all-cause LRTI hospitalizations.
4. Small effect sizes.
5. Since the incidence of RSV hospitalizations is low after 3 months of age and no effect is observed at this time, a trial that targets healthy term infants >3 months specifically should be conducted to justify treating kids >3months.
No parent wants their child to be hospitalized for RSV. But the evidence was not strong enough for me to recommend prophylaxis for all babies < 8 months.
Perhaps a breastfed healthy term baby staying at home for the first 3 months of life does not need this extra shot added to their immunization schedule? Unfortunately, universal vs. targeted prophylaxis continues to be the preferred public health strategy.
[i] Efficacy calculated as 1 minus the relative risk.
|
 | A guest post by
|
Great summary of the evidence! I had done some reading about the maternal vaccine and the monoclonal antibodies for infants while I was pregnant and decided to decline both if offered. My son had a 2 month check up this week and it was recommended he receive Beyfortus. When I asked the doctor about the benefit vs risk, she had no idea.
Still getting my jaw off the floor re 50 euros a dose in Europe vs $1,300 here.