
NYTimes is now Pro-Obesity & Mt Sinai Med School Says Weight Loss is Racist: Medicine is Drowning in Deranged Ideas.
We need to stand up for common sense in medicine

This week, I read two things that are emblematic of just how common sense is in a decline in American medicine. They are both on the topic of obesity. First, let’s remind ourselves that obesity is a problem that is rapidly getting worse in America. We are fatter than ever before.

Now, if I were in charge of federal budgets, I would commission dozens of large, 10k-100k randomized trials of different dietary and exercise strategies, different health advice, different incentives for grocery stores (cluster design), parks (cluster), bike lanes (cluster), and many other interventions.
My trials would be powered for hard endpoints (CV events, death, etc), with supplementary studies powered for HRQoL and softer endpoints among the young. If medications are tested, particularly in younger people, I would expand the sample size to 100k+, and extend duration of follow to look for rare and relevant safety signals that might be missed.
You know what I wouldn’t do: Deny that it is a problem.
Exhibit A: Mt Sinai school of medicine has emailed the entire school, arguing that diet culture is racist. I attach the full email at the bottom of this essay, so you can see for yourself just how ridiculous it is.

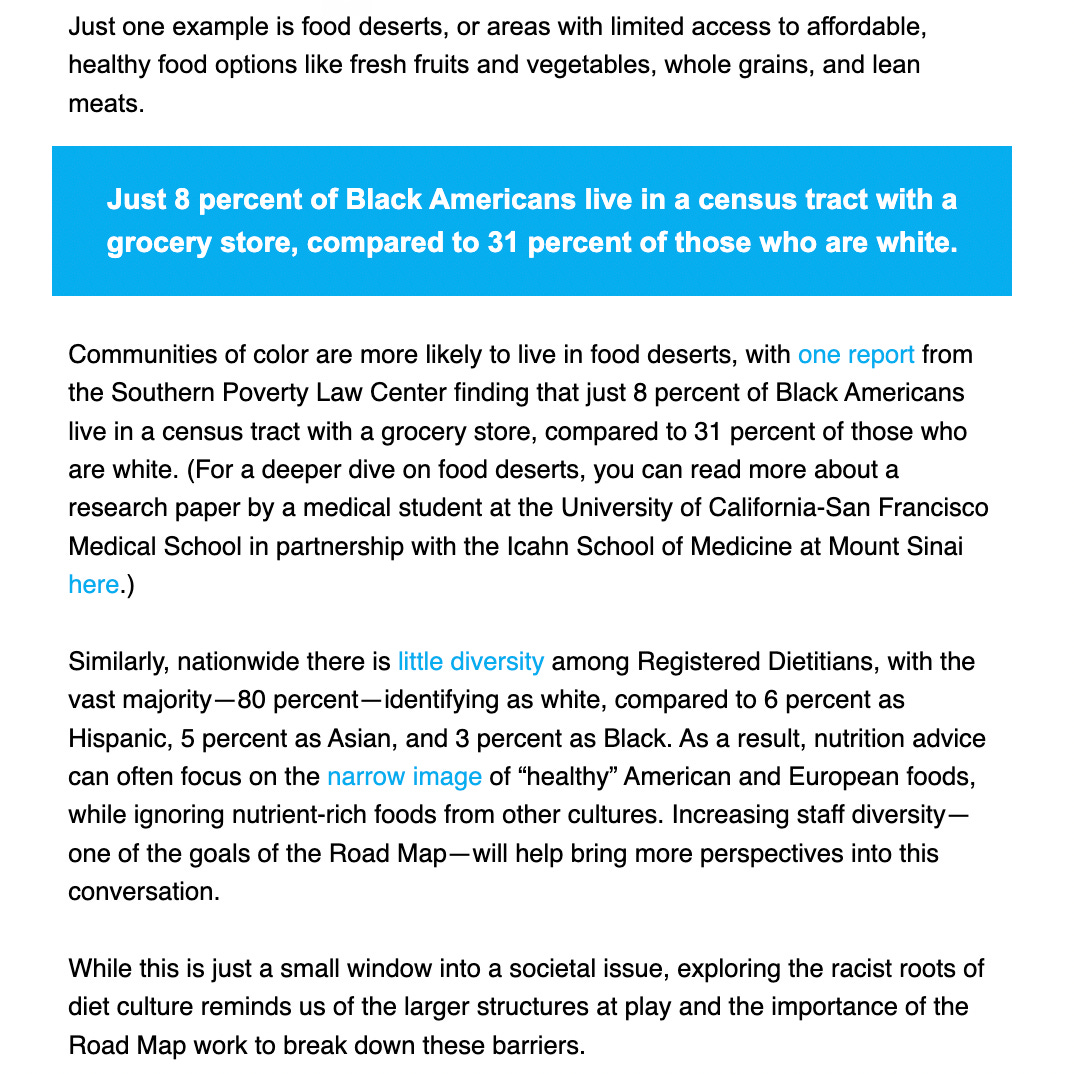
The argument made is that the idea ‘it is good to be thin’ is itself racist, and the general argument advanced is that Black and Brown communities often live in food deserts, and there are fewer dietitians who are familiar with preferred foods of these groups to give relevant advice.


But the authors are making a flawed argument. Yes, we should work on making healthy foods equally available to all Americans, irrespective of race and wealth. And yes, we should work on having a variety of dietary advice that pleases all palettes. And yes, we should study the optimal weight and BMI for different people by race or ethnicity, body type and other factors, but the idea that ‘being thin is healthy’ is not racist. The path to get there may be harder for some people, but the goal is sound for all races.
Finally, why are they emailing this to the entire school of medicine? Why is there no rebuttal? What are they teaching medical students? (is it teaching if you don’t entertain debate on demonstrably false claims?)
Exhibit B: The New York Times has an essay critical of the New Pediatric Obesity guidelines. My first thought— was good! I was also critical about putting a 12 year old boy on a GLP1 agonist weight loss drug in perpetuity. Does he take it for 50 years? What AEs happen with 50 years of treatment? But I was wrong!

The article was critical of the very fact that obesity is bad.
The author argues that Obesity is not a problem in kids. And that we could embrace different weights. She even gives the most bizarre advice I have ever seen for an Obese person: eat more calories!
Have we lost our minds?
Of course, no one should be teased or mocked or treated poorly because of their weight. And children are sensitive, and issues of weight should be discussed compassionately and carefully, but if you want to claim that it is good that kids’ weight is rising, and obesity is the highest it has ever been— you are out of your mind.
It is neither racist nor bad medicine to try to compassionately get someone who is overweight or obese to lower their weight. Their blood pressure may fall; They may have more energy; COVID is less likely to kill them; and they may live longer.
Just how to best counsel them is an open question— requiring RCTs (and huge ones)— but the idea that this is a task worth taking is settled. Obesity is unhealthy; The rise in obesity is bad for health and humanity; and we have to tackle it.
Minorities and poor people need extra support, but they do not need to be told the very premise of losing weight is racist or unnecessary. Kids need much better evidence— and, yes, the AAP is a terrible organization that just makes things up— but the idea obesity is harmful to kids is true.
Medicine is suffering from a brain parasite: the ideas expressed in both these essays. Trying to lower weight among those with unhealthy weight is a racist goal, and we should be happy with surge in obesity among children—- These are clearly ridiculous ideas that are being presented as if they are fact with little push back.
Common sense in medicine is dying.
Full Exhibit A:

Fat and trans is are cash cows for big pharma drugs. They need new sources of revenue now that covid is fading. Always follow the money: https://yuribezmenov.substack.com/p/how-to-do-no-harm-part-2
Vinay, This is well done. And goes hand in glove with all of the demographically-driven drivel we have been forced to consume over the past five years from organizations (AMA, Federal Government, AAP, you name it) that used to know better. I am a hematologist and telling me that it is racist to point out that Sickle Cell Anemia is primarily a disease of black people is insane -- but that is the standard mantra these days.
As soon as one departs from the long-standing requirements for a medical student to: 1) be of above average intelligence, particularly at mastering medical information AND 2) have an overriding passion for caring for the patient sitting in front of you NOW, health care just becomes politics and increasingly an exercise in idiocy. Covid has shown this in spades, but there is plenty more to go around.
I place much of the blame on the LCME, the accrediting agency for medical schools, which has forced all of this drivel to become the only acceptable mantra to teach. It will take a new accrediting authority and a concerted effort by doctors like you (and me) to turn this around.
I fear that these excellent Substacks that are clearly correct but resoundingly ignored by the Government and those who are lap dogs to the government (AAP, AMA, etc.) will not be enough to stop the slide. You have a far bigger bully pulpit than I and your writing is incisive -- but what difference is it making? That is the question we need to answer...and soon.
Also, I notice that you have stopped posting on Brownstone. That is too bad because they have a very broad worldwide readership, and your work needs as much exposure as possible.