
Perhaps the Strongest Benefit of GLP1a drugs is...
Reports from an ongoing trial in NEJM has flown under the radar but might show a major discovery in Medicine

Three professors, writing in the Lancet, estimated that the global prevalence of the condition is 25%. A modeling study predicted that its prevalence will rise sharply in the coming decade.
The condition has a terrible name. It’s called metabolic dysfunction-associated steatohepatitis (MASH). That’s its new name. The old names, non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH) were not much better.
Basically, these are the long names given for complications of fatty liver. Too much fat in the liver creates inflammation, then fibrosis (scarring), then cirrhosis or liver cancer.

You notice the problem of fatty liver when you fly back from Europe and walk into an American hub airport. You just spent a week in a European city where it’s rare to see an obese person. Then you arrive in Detroit, Charlotte, Atlanta and nearly every other person is overweight or obese.
MASH occurs almost exclusively because of obesity and its associated diabetes. While most of the deaths in people with MASH are cardiovascular-related, liver-related outcomes occur in more than 10% of cases. Since the number of people affected is so large, that’s a lot of bad liver-related outcomes.
The Study
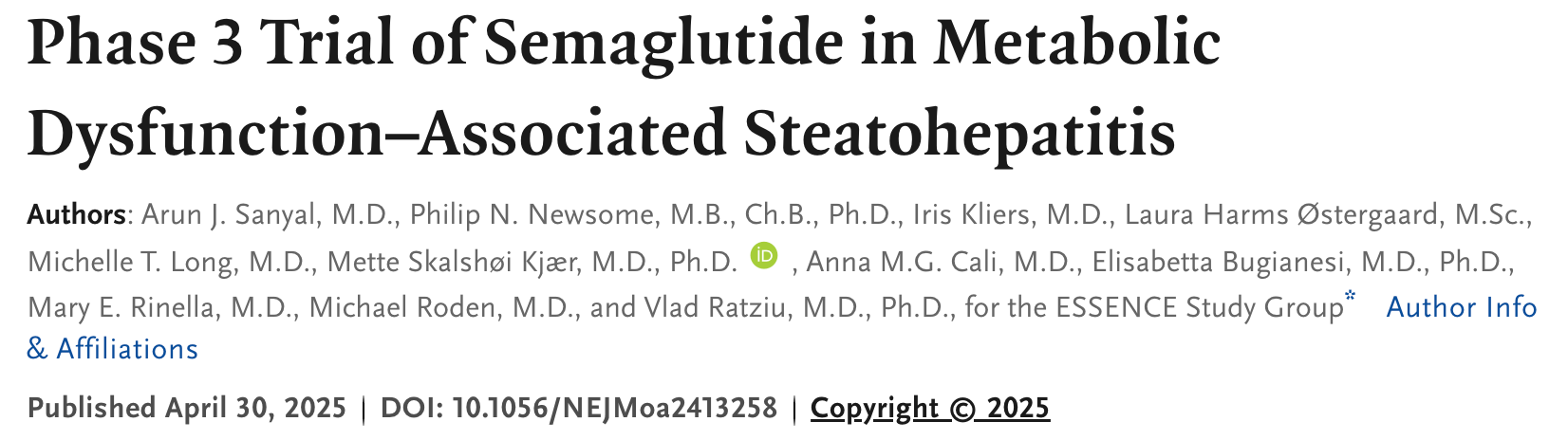
NEJM published the first report of the ESSENCE trial, an RCT comparing semaglutide vs placebo to treat patients with non-alcoholic fatty liver disease. It is a two-part trial. Part 1 has resolution of steatohepatitis without worsening of liver fibrosis and reduction in liver fibrosis without worsening of steatohepatitis as the primary endpoints. The trial is ongoing and Part 2 will measure clinical outcomes.
The trial enrolled only patients (N ≈ 1100; 2:1 randomization) with documented inflammation on liver biopsy. Patients were young at age 56 and more than half were females. The mean BMI was 34-35.
The results were highly positive. Here are images of the primary endpoints.
Secondary endpoints all favored semaglutide. Liver stiffness, fibrosis markers and liver enzymes (AST, ALT) all improved in the active arm. Glycemic indices, blood pressure, insulin resistance, CP and lipids also improved on semaglutide.
Adverse events leading to premature trial discontinuation occurred in 2.6% of the patients in the semaglutide group and in 3.3% of those in the placebo group.
Comments
I am not a liver expert but this looks like a major breakthrough in a largely silent disease.
The FDA recently approved a drug to treat this condition, called resmetirom, which has mild cholesterol-lowering effects, but no known CV benefits.
GLP1a, on the other hand, have proven benefits beyond liver disease. In the SELECT trial of obese patients with established heart disease semaglutide reduced major adverse cardiac events by about 20% over placebo. The SUSTAIN-6 trial found similar risk reductions in MACE endpoints in patients with diabetes and obesity.
GLP1a drugs, therefore, provide a more holistic treatment for patients with fatty-related liver disease, which is huge, because most patients with MASH die of CV causes.
When I look at these results, the verb shred comes to mind. Semaglutide seems to shred the bad effects of fatty-related inflammation on the liver.
That said, this is week 72 of a 247-week outcomes trial. And liver inflammation seen on a biopsy is a surrogate outcome.
I would normally say we have to wait for clinical outcomes. But I cannot see how this trial finishes. Given the GLP1a ability to reverse fibrosis and improve nearly every marker of metabolic dysfunction, I expect this trial will be stopped early for efficacy.
I often report here on problematic studies, but I thought it was important to cover studies that show potential breakthroughs. And this looks like a major advance for a condition that affects (literally) billions of people worldwide.
Or we could eat like Europeans and not need drugs
As much as we’d like to believe in miracle drugs, they always lead to the same question: how do they address the root cause of the metabolic dysfunction? Just like Metformin (for diabetes), these drugs improve lab values but at what cost? Eliminating seed oils and highly processed foods, addressing gut health, ensuring enough rest and sunlight and movement, adjusting macros and micros for optimal nutrition to address deficiencies… true healing takes WORK and effort. Big Pharma wants you to believe a shot or pill is the answer … and nothing could be further from the truth.