
Preparing to Battle the Computers

We at Sensible Medicine have been a bit overwhelmed by submissions about ChatGPT. “AI” seems to have replaced “In the Age of COVID” in every title. Thus, we present you with a call to arms, stimulated by a last generation technology.
Adam Cifu
Practicing emergency medicine, I’m no stranger to mediocre algorithmic medicine described by Vinay Prasad in his recent post about Chat GPT’s potential influence on medical practice. I’m on the receiving end of clinicians and patients with “algorithm-dependence syndrome” - the uncritical use of computer “decision support tools” and flow charts - that result in unnecessary emergency department visits. The well-meaning but inexperienced clinician or worried person at home doesn’t have the medical experience to critically evaluate the computerized information in which an algorithm ends with: “go to the Emergency Department.” Algorithm dependence is one of the many reasons Emergency Departments continue to see high volumes of non-emergent patients.
Even before the internet and decision support algorithms, we had EKG machines with sophisticated software to measure rate, rhythm, intervals, and detect acute myocardial infarctions and dangerous cardiac dysrhythmias. Given that chest pain is a common complaint, and one whose mismanagement can have devastating consequences, we have clear guidelines in Emergency Medicine. Patients presenting with chest pain have an EKG that is immediately reviewed by an attending physician.
During our training, many of us were taught to read the EKG with the computers interpretation covered. This helped to improve EKG literacy and acknowledged that both human and computer are fallible. Doctors might miss a subtle or rare finding. A computer, “unaware” of the clinical situation might over call (early repolarization read as a STEMI in a young healthy person) or under call (missing a widened QRS in a patient who missed dialysis) findings on an EKG.
On a recent shift, I logged into the EHR and signed up for my first patient, a 55 y/o man with chest pain. The tech handed me the following EKG:
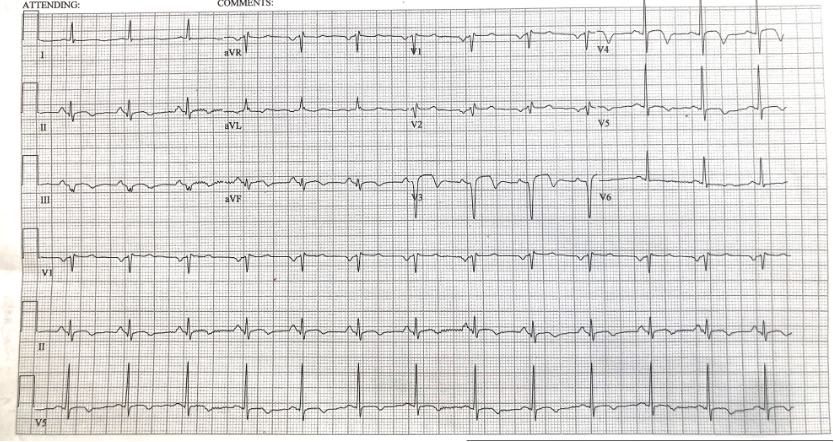
The computer read this EKG as follows:
· Normal sinus rhythm
· Possible left atrial enlargement
· Anterior infarct, age undetermined
· T-Wave abnormality, consider lateral ischemia
After I confirmed with the patient that he was having chest pain, I activated the ST elevation MI (STEMI) alert. The patient went to the cardiac catheterization lab where he was found to have multi-vessel coronary artery disease. He had a successful triple vessel bypass the next day.
Was the computer algorithm correct to not add the label **** STEMI**** across the top of the EKG because the EKG does not have 1-2 mm ST elevations in 2 contiguous leads? Was the computer misled because the patient looked fine, had normal vital signs, and was calmly reading his phone when I walked in the room? Should the computer have been more alert because the patient was a middle aged man with chest pain?
The patient’s troponin drawn at triage came back at 16,388 ng/L (normal <77 ng/L). Had I not acted immediately, the elevated troponin would have triggered the process soon thereafter. This patient was stable and would have probably done just as well even with a delay caused by a computer EKG misread. But other patients deteriorate quickly and sometimes the lab draw or analysis is delayed. The EKG read “anterior infarct, age indeterminate” and “T-Wave abnormality, consider lateral ischemia” – though factually correct -- may have delayed care if a clinician was only looking for the ***STEMI*** read by the computer. The patient could have sat in the waiting room for hours if the department had long delays and his blood couldn’t be drawn right away.
In the unpredictable world of emergency medicine, I’ll take this as one more victory of doctor against the machines. I look forward to sparring with Dr. Chat GPT in the future.
Carrie D. Mendoza, MD is the Director of FAIR in Medicine with FAIR, the Foundation Against Intolerance and Racism, a non-partisan nonprofit advancing fairness, understanding, and our common humanity. She lives in Chicago with her family and practices emergency medicine in metro Chicago and southern Wisconsin.
 | A guest post by
|
I don’t think that Artificial Intelligence will ever be able to beat experienced physicians who are able to read subtle symptoms and look at the whole picture.
Good example to support use of AI in urgent care scenarios of a certain type, yet the huge challenge yet to overcome will be discerning case types when AI should not loom too large, if at all, in the overall choreography of particular diagnosis and therapy selections (including timing). How such issues will get hammered out is totally up for grabs. I foresee creation of new journals, new national meetings, maybe even new "board certifications" for doctors/nurses and {God help us} a large blizzard of new bullshit and new buzzwords and new jingles. I even foresee creation of yet another managerial niche in modern healthcare temples: AI Officer, perhaps one for every specialty. Not kidding. And do not forget that the Bean Counters with the green eyeshades will no doubt have a way to lobby for putting into every single AI "software template" various concealed gimmicks that will be carefully crafted LOSS PREVENTORS (i.e. money-saving sidetracks).