
Primary prevention, statins, lottery effects and misinformation that is not actually misinformation

Today we consider the communication of a benefit of a medical intervention.
It’s not as simple as you might think. As an offshoot we also consider the term misinformation.
When you break a hip, burst an appendix, or have an acutely clogged coronary, treatment benefit is obvious. The NNT is 1.
When you take a preventive medicine, it is less obvious.
Clinical trials measure outcomes in two groups (treatment and placebo). The result is an average effect size, expressed as a relative or absolute risk reduction or increase.
Let’s take the HOPE trial of statins for people without heart disease. More than 12,000 patients were given statin or placebo. The relative risk reduction with statins was 24% and the absolute risk reduction was 1.1% (3.7 vs 4.8%).
One way to express this difference is to use the NNT or number needed to treat. 1/1.1% leads to an NNT of about 91 patients. Meaning we treat 91 patients so that 1 avoids a nonfatal event, such as MI.
There are problems with the NNT, because it’s likely that LDL-lowering from statins has a legacy effect and the risk reduction grows over time after the trial ends
Many doctors were commenting on this clip of UK cardiologist Aseem Malhotra speaking with Joe Rogan.

Canadian cardiologist Martha Gulati quote Tweeted it as follows:


Many others also called it misinformation for saying the average lifespan gained is only 4 days.
I am not sure Dr. Malhotra’s claim is misinformation. It may be distorted framing, but calling it misinformation is a serious charge.
Three Danish authors estimated the survival gains from a summary of statin trials. Since most of the benefit from statins is prevention of non-fatal events, the survival gains are in the range of 5-22 days.
I suspect this is where Malhotra got his data. So, he is not exactly wrong. Hence his statement is not exactly misinformation.
But his framing is off.
The first way this framing misleads is that statin-induced lowering of cholesterol has a legacy effect. The trials go for 5 years and the curves separate over time because longer exposure to lower cholesterol reduces blood vessel disease. It’s likely that survival gains are greater over the years. Though how much so is speculation; and those who estimate statin benefits over 20-30 years speculate a lot.
The far more interesting idea in framing preventive therapies is to consider the puzzle laid out in one of my favorite pieces on statins—God and Statins by Dr. Saurabh Jha. In this witty piece, Jha exposes the challenge of applying average effects to individuals. If the NNT is 91, are you the 1-90 or 91?
Distribution of Lifespan Gains
The group of Darrel Francis at Imperial College published a cheeky paper on the distribution of lifespan gains from a primary prevention intervention.
For this modeling paper, they estimated that a primary prevention therapy would reduce outcomes by 30%. They then calculated mean lifespan gain, and then the distribution of lifespan gain.
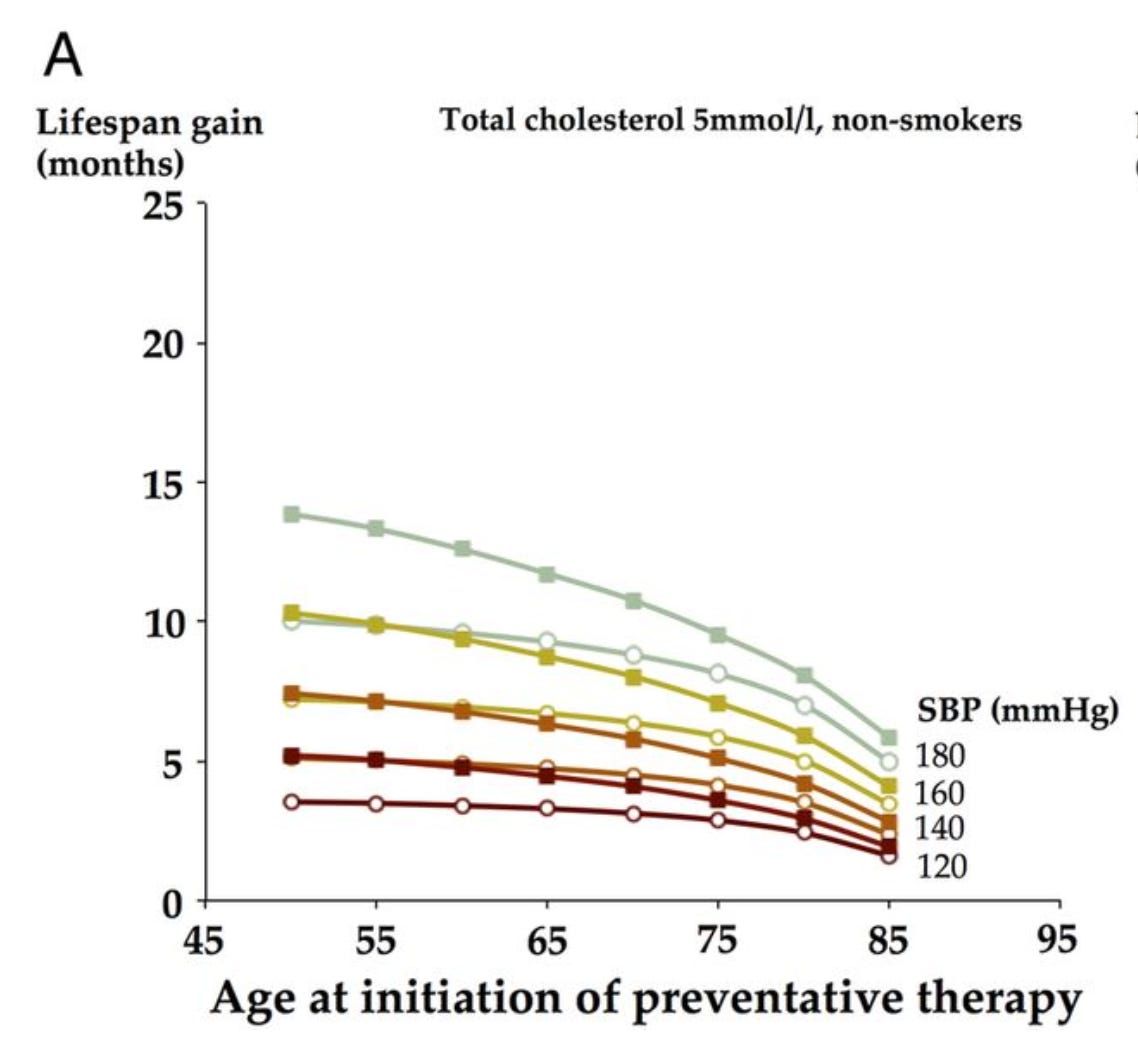
For a lifetime of prevention (not 5 years in a trial) the mean lifespan gained is in months. The higher the blood pressure and earlier one starts the more the gain.
But. Wait. These are still average gains. Here is where it gets really interesting. Look at this figure:
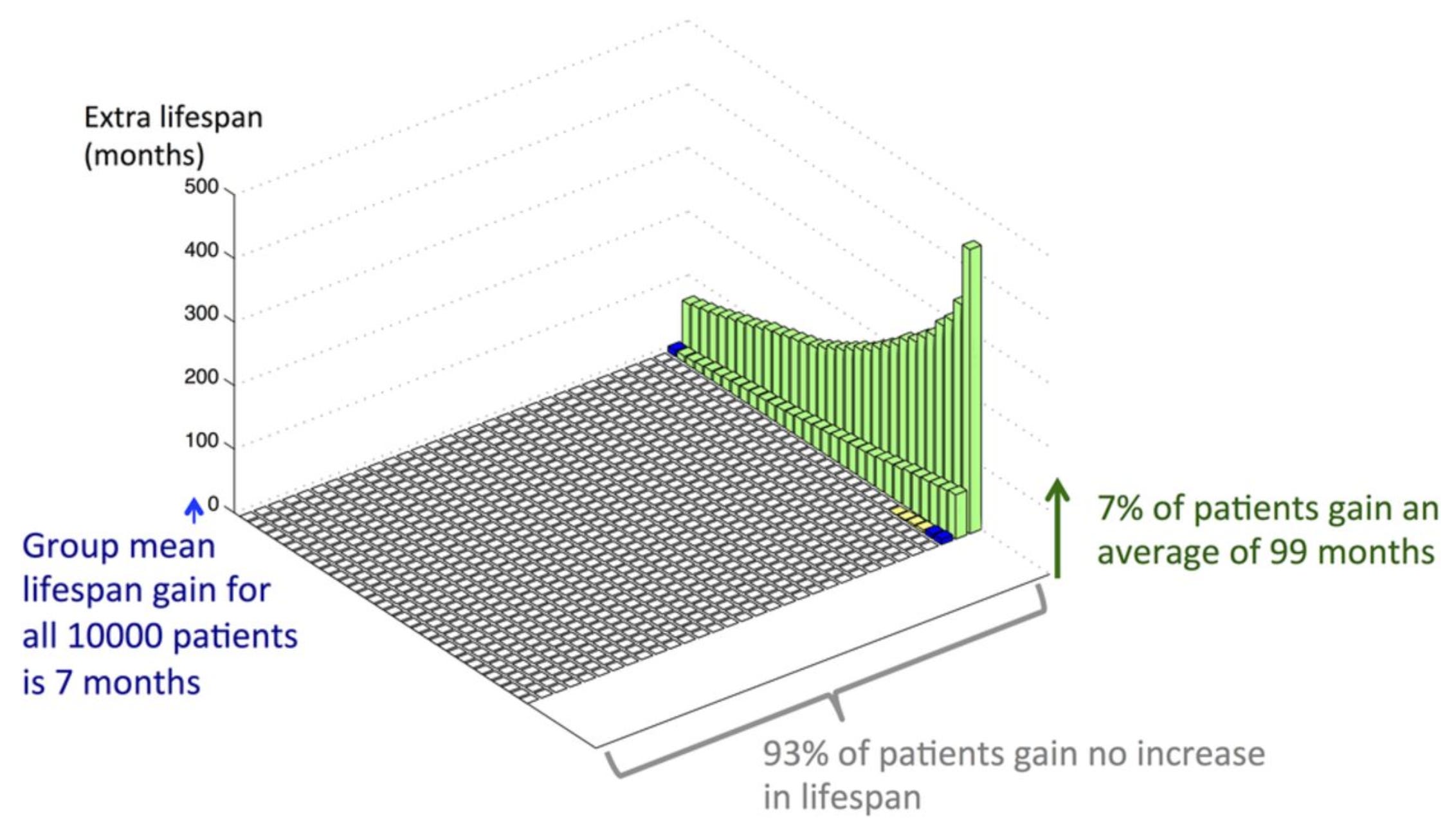
This depicts the distribution of lifespan gains from taking a daily preventive therapy with a 30% risk reduction for men with an average cardiac risk starting at age 50.
Notably, the great majority of men (93%) gain no lifespan while the minority that do gain, gain much more than the group average.
For example, for a 50-year-old, non-smoker, non-diabetic man with average cholesterol and BP, mean life expectancy gain is 7 months starting preventative therapy. However, among such individuals, 93% gain no extra lifespan, but the remaining 7% gain an average of 99 months.
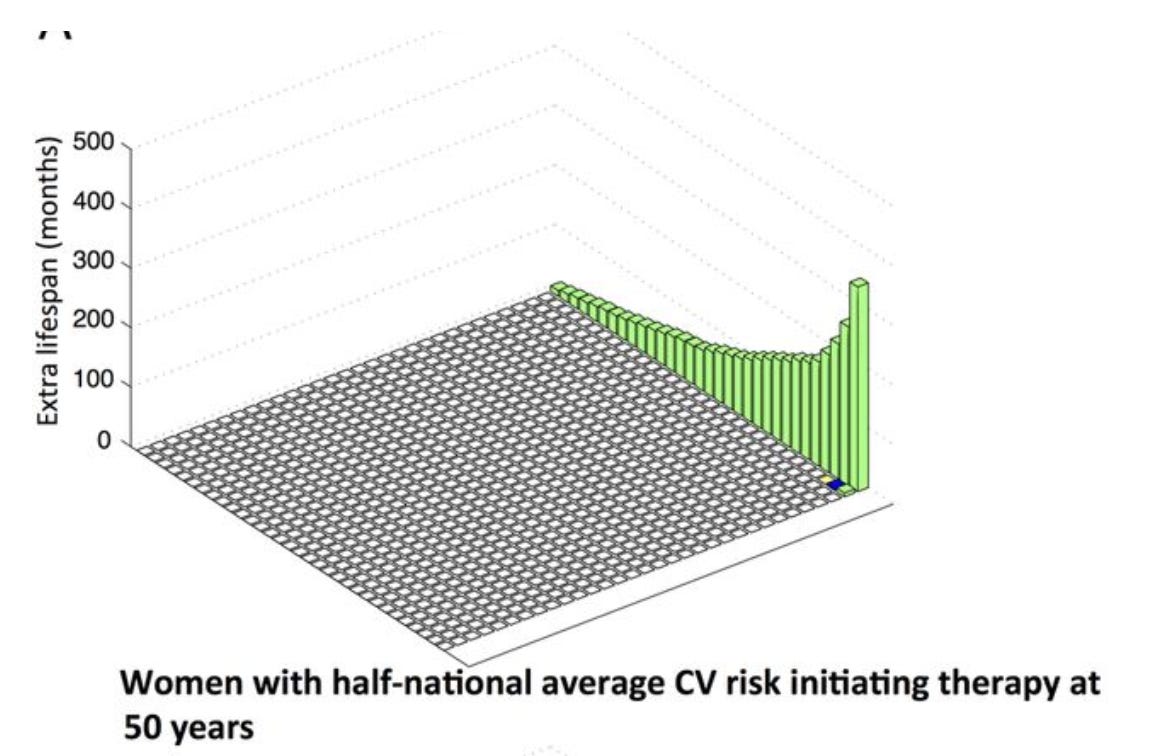
These distributions change according to baseline risk and when a primary prevention therapy is started. For instance, for women with half-national average CV risk initiating therapy at 50 years, the mean life expectancy gain is 3 months, 96.6% gain no extra lifespan, but the remaining 3.4% gain an average of 92 months.
This is a complex modeling paper. But I think it bridges Drs. Jha’s God and Statins piece and the notion that average lifespan gains are true numbers but not representative of how probability works in preventive therapy.
One more example and then I will close. One of the worst cardiac conditions is unstable ventricular tachycardia or fibrillation. Another name for it is cardiac arrest.
The AVID trial compared ICDs to amiodarone. AVID established the ICD as the superior treatment as it reduced death by a whopping 39% in relative terms. The absolute risk reduction was huge at 8%. An NNT of only 12 patients—much lower than statins.
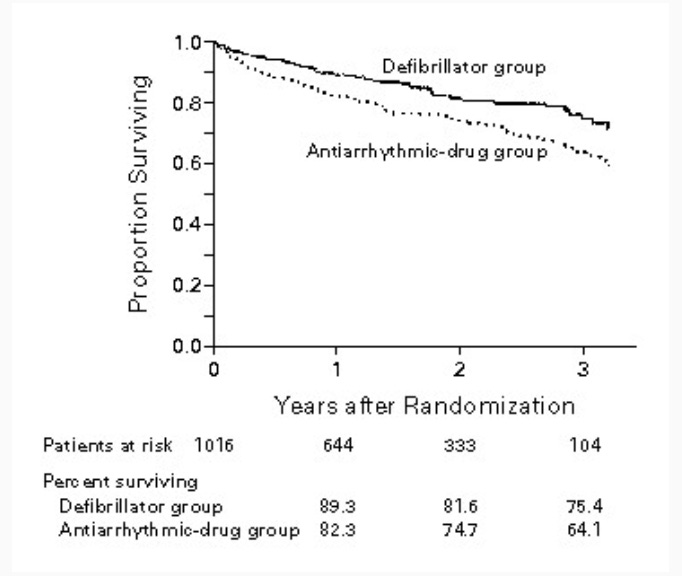
But look at this pull quote from the NEJM paper:
The average unadjusted length of additional life associated with cardioverter–defibrillator therapy was 2.7 months at 3 years.
How can a machine that terminates a lethal arrhythmia and has a massive average effect size only increase lifespan by 3 months?
Conclusion
The average survival gain is low because most people who have an ICD never have a cardiac arrest and the device provides no survival gain. Same with statins as shown in the UK paper.
But a fraction of patients get a huge benefit. To wit: If a statin stops a massive MI at age 51, you get three decades more. If an ICD stops a cardiac arrest, you may also get years to decades to live.
But when you calculate “average” effects over the entire population, it is quite small because most people don’t benefit.
As a patient considering a therapy, you don’t know which group you will be in. You have to balance the downsides (disutility) of taking a daily statin or having an ICD.
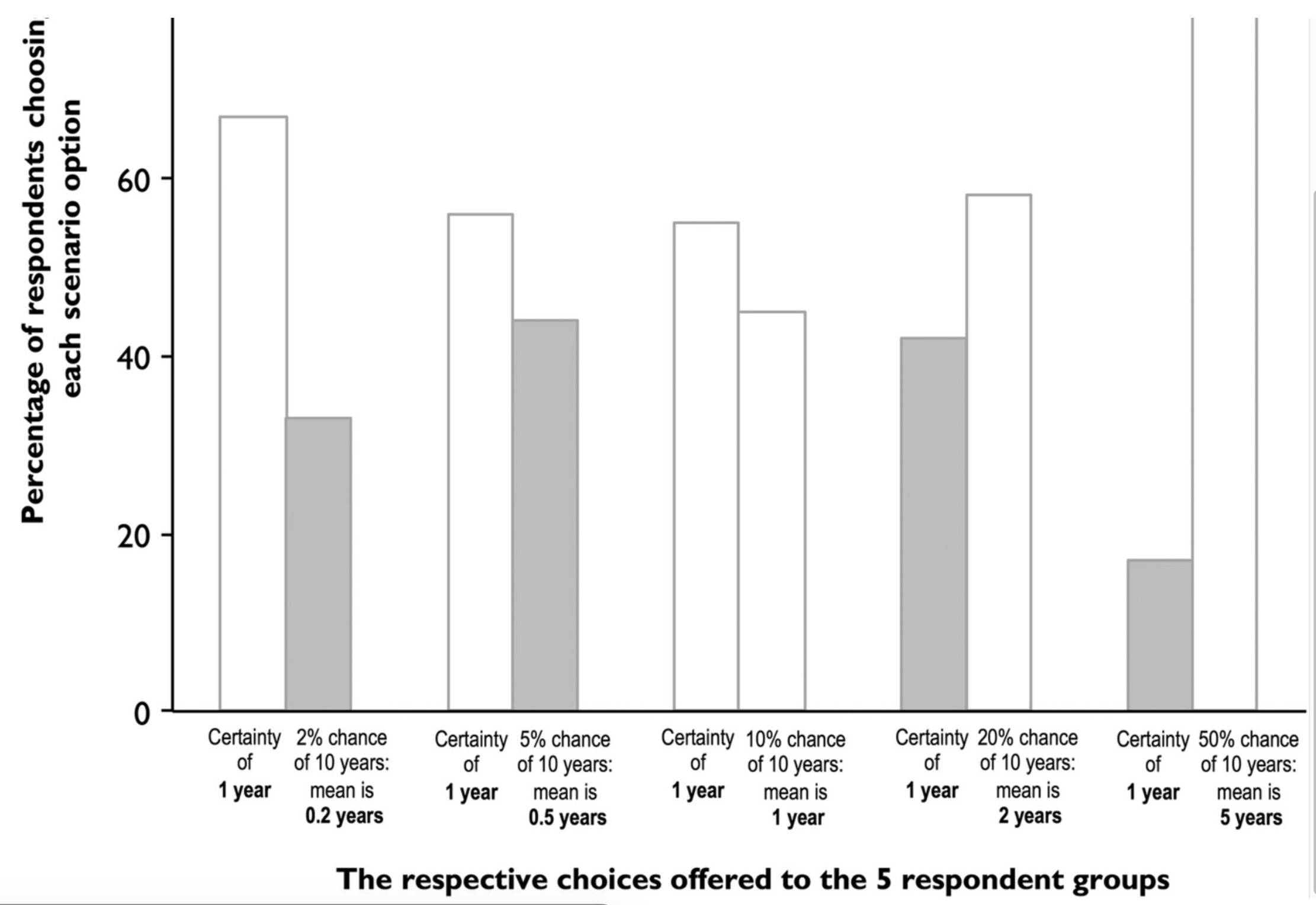
The UK team actually went out into London tube and asked random people their preferences on maximizing lifespan. Each person chose between the certainty of 1 year gain or a % chance of 10 years gain.
You can see (in the gray bars) that many people chose numerically lower mean life expectancy.
To conclude, the communication of effect sizes of preventive therapy is complex.
I often hear such things as: this patient needs a statin, or needs an ICD. This is soft thinking because most people who get these therapies don’t benefit. But some do—and they benefit a lot.
Our job is not to hollar misinformation but instead explain the nuances of how preventive medicine works.
Calling something misinformation that is not misinformation is one of the ways we lose trust as a profession.
Dr. Mandrola, a little bit of good news. You DO NOT have to worry about losing trust as a profession. After the COVID and vax debacle, that ship sailed. I, now, have ZERO trust in the Big Medicine machine. But it's also why I subscribed to Sensible Medicine. There's some sense of hope that the trust can be rehabilitated. But with every step forward, there's some shill like Neil Stone that keeps harping on mRNA C19 vax and how it did and will save humanity. So I take another giant 5 steps back.
Well put. In some ways, one could conceive of this as being like insurance. One hopes to never have to use their homeowners insurance, but if you do need it, the benefit of being insured is often substantial. That’s probably a more honest framing of taking a statin, for example, that still conveys the benefit.
Nice article!