
Public health experts went on Twitter between May to October 2022 and promoted blatant misinformation about Monkeypox
We explain our new paper



In the summer of 2022, fears of monkeypox ran rampant. A number of public health experts turned to Twitter to provide commentary. We went through those tweets and judged them based on accuracy. The results are a damning indictment of public health. Here are the highlights, but check out the full paper here if you haven’t already.

In case you’ve forgotten, think back to the summer and fall of 2022. Numerous individuals, especially those in public health, medicine, and the academy, made predictions that monkeypox would spread throughout schools, endangering children and young people.
Others suggested that measures like masks and social distancing were needed in classrooms to advert the virus. Given that monkeypox was spreading by gay men during sex, we wondered exactly what they thought masks were doing.
Some ‘experts’ even proposed delays to the start of the school year, or in extreme cases, school closures. Such measures would further damage a generation of kids already hurting.
If your memory is escaping you, please see some more memorable tweets below (credentials of author listed in parenthesis):
Children with monkeypox: This is the tip of the iceberg (as symptoms can be mistaken for other rash in kids) & we expect the numbers to rise. With school opening & shortage of vaccines, these numbers will ⬆️in the fall unless we expand testing & vaccine. (MD MPH Professor)
When you pen an op ed saying #monkeypox cases are doubling every two weeks… and a few hours later you find out they are now tripling…
🙊 🚀 The monkeypox emergency is going to affect schools, colleges. Be ready (Former Surgeon General MD MPH)As predicted, Monkeypox started as an STI, but it’s not staying that way. What does this mean? Time to plan to prevent not one, but two dangerous viruses from spreading in schools and daycares.
Denying this unfortunate reality will not make it go away. (MD)All of #MedTwitter has worried about this, but I hoped it would not happen so soon. I hope every childcare facility & school system is thinking now about how they will handle a #monkeypox exposure or outbreak. (MD)
The @CDCgov wants to lift Covid restrictions in schools just as Monkeypox starts spreading in schools. We are the most resourced idiotic country when it comes to managing the public health. Happy Back to School! (MD)
Public health officials need to get ahead of this issue & imminent school return -> how do we have appropriate guidance & hygiene measures so we don’t see outbreaks among children in schools? Monkeypox spreads mainly through prolonged skin-to-skin contact (PhD Professor Global Public Health)
New world record — More than 1,000 daily #monkeypox cases (7 days average). Those who said #MPXV would fizzle out soon are plain wrong. This fall school year will need radically new / more safety mitigations. Figure by @Antonio_Caramia (Epidemiologist, ScD)
Monkeypox, if not rapidly contained, will inevitably spread among kids in daycares, schools, and sports leagues. The vaccine currently being used won’t be the silver bullet since supply is limited and it wasn’t studied in children so it’s not approved for <18s. What’s the plan? (MD Professor)
I honestly cannot imagine that it wont spread in schools given that no one seems to be doing anything to stop the spread. I do not at all understand how people can say otherwise. Unless they think men who have sex with men are never parents? Or they do not understand transmission (referencing Mpox) (comment) (ScD Epidemiologist Professor)
I hate to tell you all this, but #covid19 is still a pandemic, and now #monkeypox is too. And both are gonna get a LOT worse before they get better… just wait till schools - including colleges- reopen in a few weeks… 🤦🏽♂️ (Former Surgeon General MD MPH)
Maybe you are thinking (as we were), why are ‘experts’ making these bold predictions? Are there data suggesting that children and young people in school are at high-risk for infection?
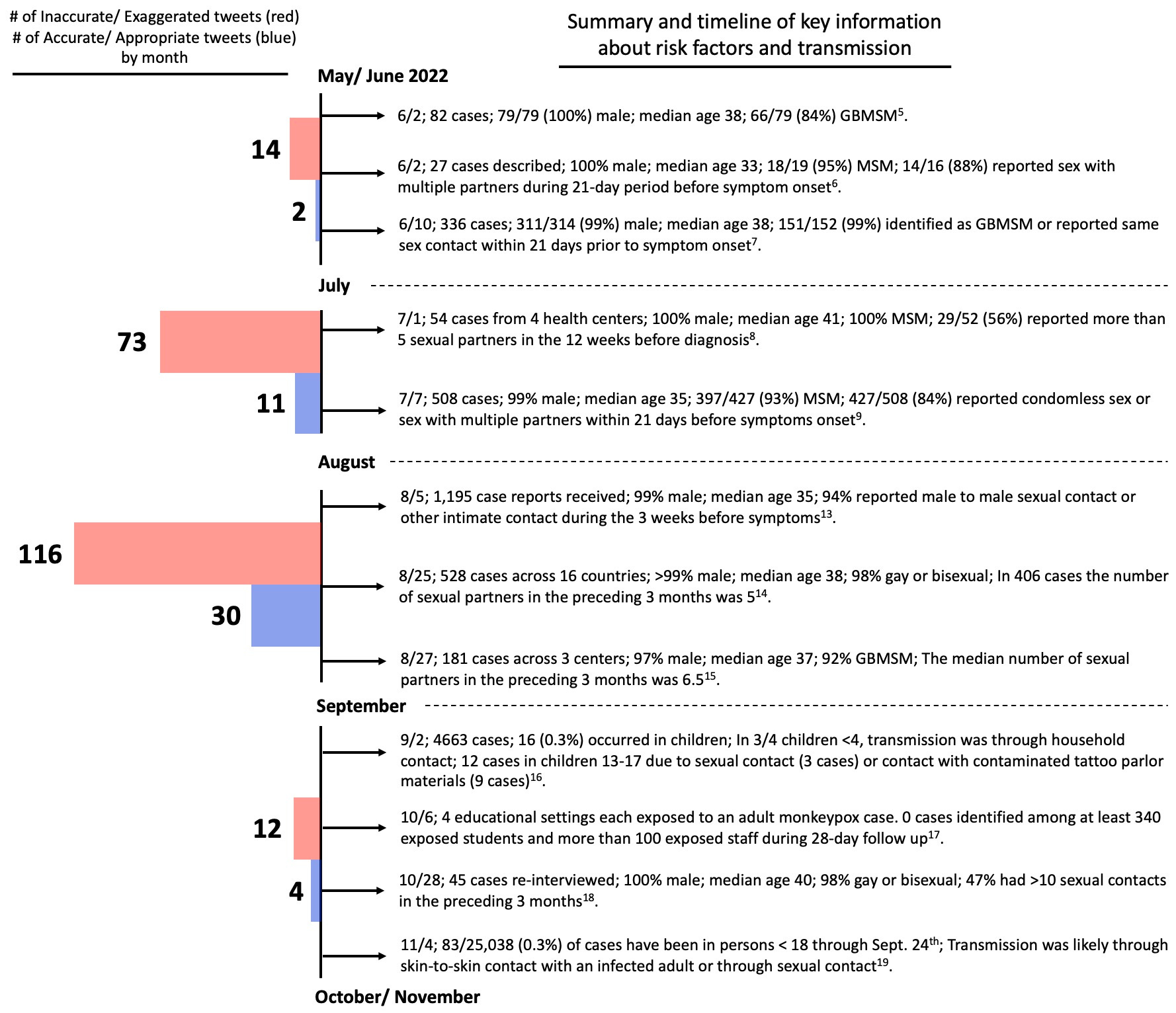
The short answer is and was no. At the time of the tweets, and as of now, there are no data indicating that schools are a high-risk environment for the spread of Mpox. In fact, it was known as early as June and July of 2022 that Mpox cases predominantly occurred in men aged 30-40 who engaged in sex with other males (see the timeline below for additional information). Moreover, the CDC found that through September 24th, 2022 only 83/25,038 (0.3%) cases were in those under 18.
The discrepancy between what was reported in the literature regarding who was at risk for infection, and the predictions made on Twitter was the inspiration for our paper.
We set out to identify all tweets by credentialed individuals** who discussed the risk of Mpox to children and young people in school and categorized them as either being accurate/ appropriate or inaccurate/ exaggerated. We quantified the number of and ratio of tweets in each group and calculated the same ratio when stratifying the tweets by the author’s credentials or degree. A few other analyses were done, and we will touch on these throughout.
** We only looked at tweets whose author fell in one of the following 4 categories: health care (MD, DO, RN, pharmacist, physical therapist, etc, including students), health reporter (health/medicine/public health reporter/columnist/expert, PhD/ MPH/ Other Ed. degree (including students), or JD (including students).
What did we find?
We identified a total of 262 tweets that met our inclusion criteria. 215 (82%) were inaccurate and 47 (18%) were accurate! This means that credentialed individuals were 4.6 times more likely to tweet inaccurate and exaggerated information than appropriate information.
When stratifying by the credentials of the author, we found the percentage of tweets that were inaccurate/ exaggerated were: Among health care professionals 95/111 (86%), health reporters 18/41 (44%), PhDs/MPH/Other Ed. 93/97 (96%), JDs 9/13 (69%).
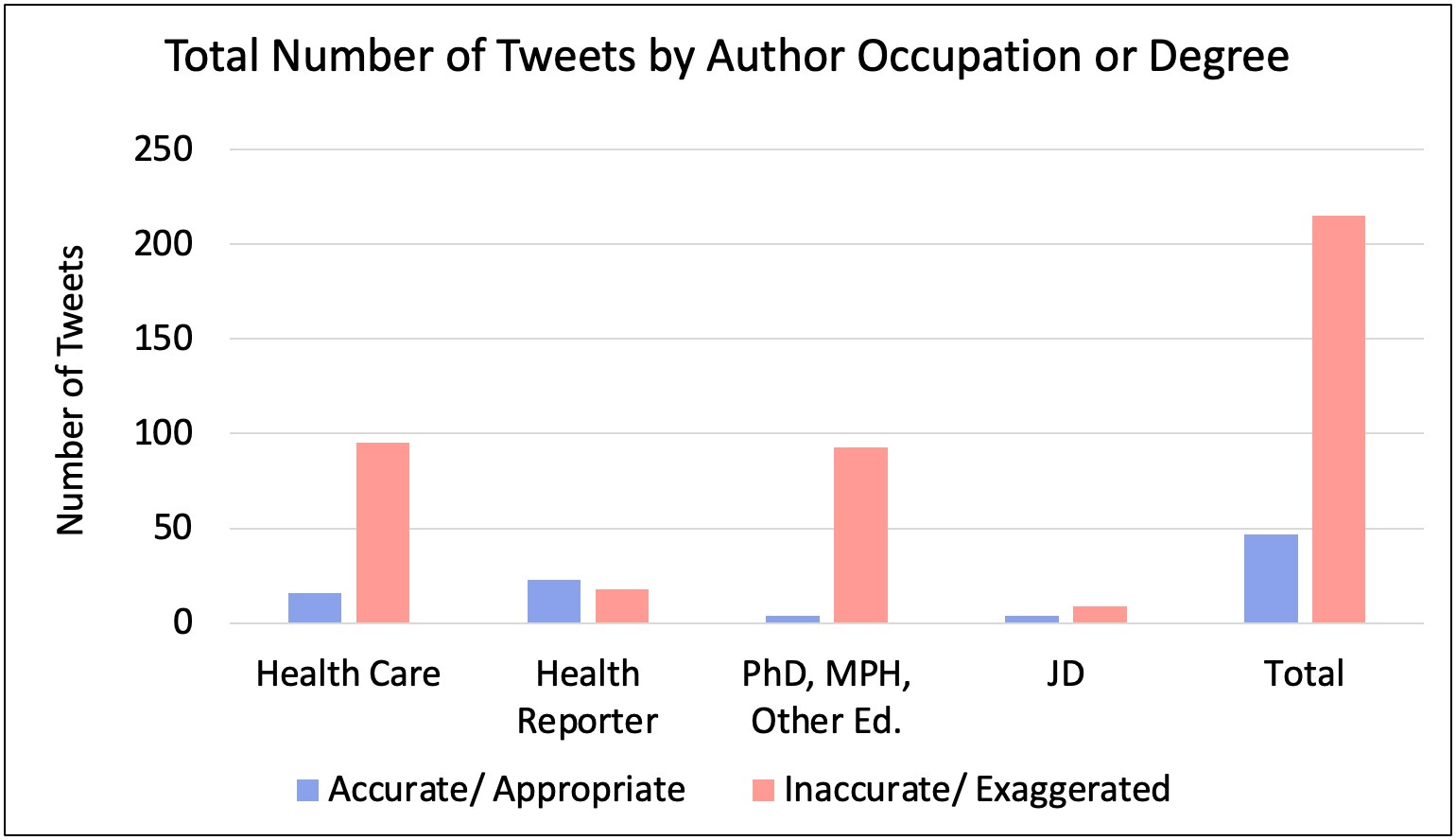
The only group that was more likely to tweet appropriate information were health reporters! However, there is one caveat – this was fueled by one health reporter who had 14 accurate tweets! Well done, Benjamin Ryan.
We don’t have an explanation for why there was such an imbalance between the number of inaccurate and accurate tweets. What’s more puzzling is that many inaccurate tweets were tweeted late in the summer (see timeline below) after there were numerous published studies describing how cases were clustered in men aged 30-40 who were mainly a part of the MSM community. This begs the question: why did perceived experts in public health and medicine feel that schools were a high-risk setting?
Since they weren’t basing their messaging off the literature, what data were they using to guide their predictions…?
We also investigated the cumulative sum of likes and retweets among both inaccurate and accurate groups of tweets over time. Unsurprisingly, we found that inaccurate tweets had an enormously higher cumulative number of likes and retweets.
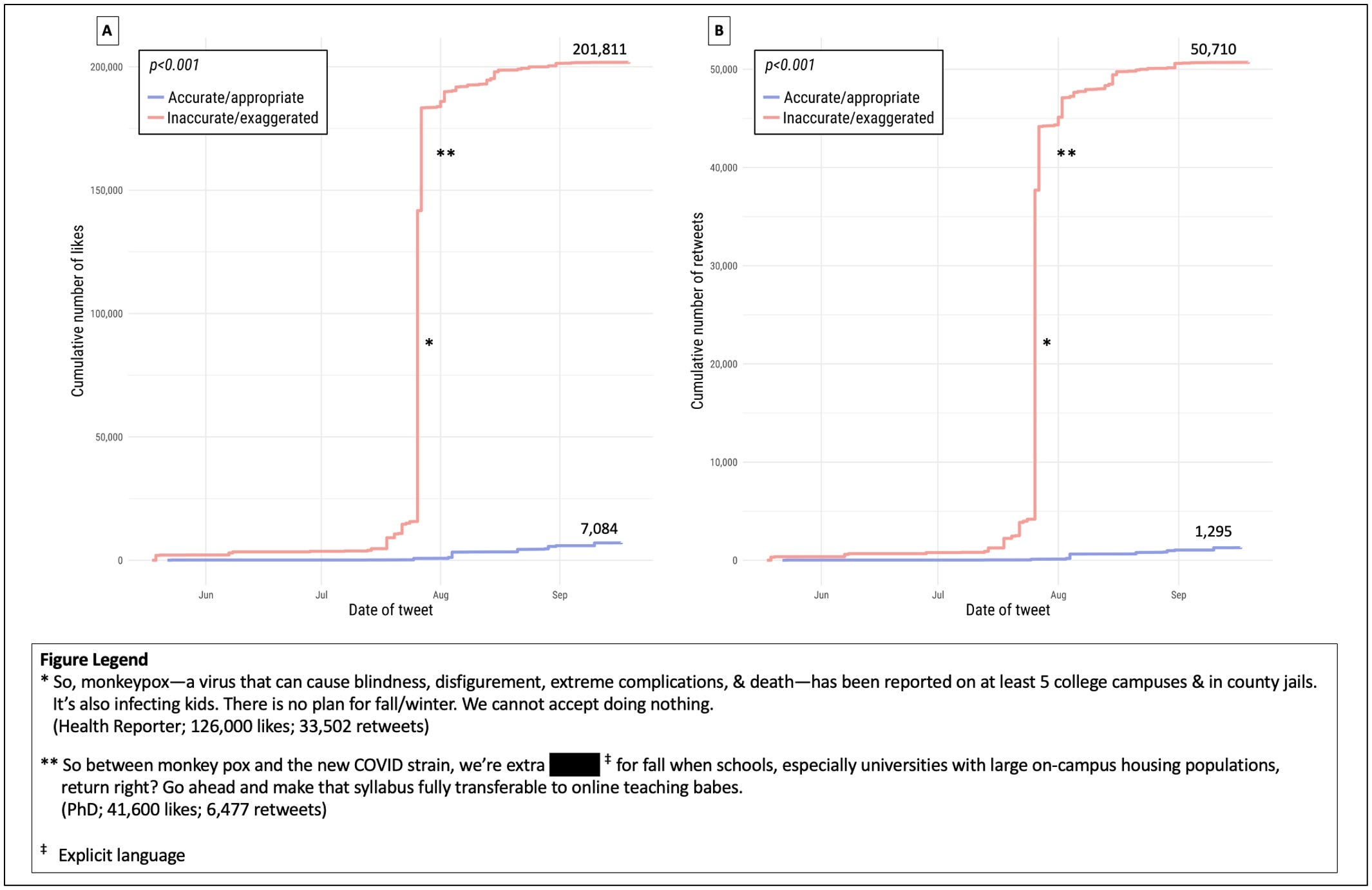
To put this in context, we estimated the relative reach of tweets in both groups. We calculated, using a share differential for followers and retweets that users on Twitter had a 974x higher likelihood of seeing an inaccurate vs accurate tweet! And 100% of the inaccurate tweets exaggerated risks of Mpox in children. This result surprised all of us, but demonstrates how Twitter can quickly magnify the spread of fear-based and, in this case incorrect information.
Immediate Implications
The majority of perceived public health experts distributed erroneous, fear-based messaging on Twitter during the monkeypox outbreak regarding the risks to children and young people in school.
Their messages were discordant with the evidence and may have created undue anxiety as well as led to unnecessary spending and energy spent trying to prevent Mpox spread in grade schools.
Broader Ramifications
Our results speak to a greater theme – public health’s self-inflicted, vanishing credibility.
Is it possible that the loudest and most magnified voices on Twitter (and perhaps social media in general) represent a minority opinion in medicine and public health but that exaggerated, anxiety-inducing messaging simply garners more attention, likes and retweets? Could this situation quickly lead to a sense of false consensus on important public health issues and diseases?
If the answer is yes, the implications of Twitter usage by individuals and the media alike may have enormous societal ramifications and health costs.
Moreover, there were no apparent repercussions to tweeting false or exaggerated information, and we uncovered a number of inaccurate tweets that were later deleted when we reperformed our initial search. Others justified their tweets later as being noble lies. One even said:
Public health experts went on Twitter during peak monkeypox, and told school kids to wear masks or maybe close school entirely, rather than telling gay men to limit new sexual partners or seek vaccination. These lies travelled around the world, while the truth was lacing up its shoes.
Public health experts complain that misinformation and rogue actors have destroyed their credibility, but our investigation suggests they are doing a fine job of destroying their credibility themselves.
Timeline References:
[5] Vivancos R, Anderson C, Blomquist P, et al. Community transmission of monkeypox in the United Kingdom, April to May 2022. EuroSurveill. 2022;27(22). doi:10.2807/1560-7917.ES.2022.27.22.2200422
[6] Perez Duque M, Ribeiro S, Martins JV, et al. Ongoing monkeypox virus outbreak, Portugal, 29 April to 23 May 2022. EuroSurveill. 2022;27(22). doi:10.2807/1560-7917.ES.2022.27.22.2200424
[7] UK Health Security Agency. Investigation into monkeypox outbreak in England: technical briefing 1. gov.uk. Published June 10, 2022. Accessed March 31, 2023.https://www.gov.uk/government/publications/monkeypox-outbreak-technical-briefings/investigation-into-monkeypox-outbreak-in-england-technical-briefing-1#sources-and-acknowledgments
[8] Girometti N, Byrne R, Bracchi M, et al. Demographic and clinical characteristics of confirmed human monkeypox virus cases in individuals attending a sexual health centre in London, UK: an observational analysis. Lancet Infect Dis. 2022;22(9):1321-1328. doi:10.1016/S1473-3099(22)00411-X
[9] Iñigo Martínez J, Gil Montalbán E, Jiménez Bueno S, et al. Monkeypox outbreak predominantly affecting men who have sex with men, Madrid, Spain, 26 April to 16 June 2022. Eurosurveillance. 2022;27(27). doi:10.2807/1560-7917.ES.2022.27.27.2200471
[13] Philpott D, Hughes CM, Alroy KA, et al. Epidemiologic and Clinical Characteristics of Monkeypox Cases — United States, May 17–July 22, 2022. MMWRMorb Mortal Wkly Rep. 2022;71(32):1018-1022. doi:10.15585/mmwr.mm7132e3
[14] Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox Virus Infection in Humans across 16 Countries — April–June 2022. New England Journal of Medicine. 2022;387(8):679-691. doi:10.1056/NEJMoa2207323
[15] Tarín-Vicente EJ, Alemany A, Agud-Dios M, et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: a prospective observational cohort study [published correction appears in Lancet. 2022 Dec 10;400(10368):2048]. Lancet. 2022;400(10353):661-669.doi:10.1016/S0140-6736(22)01436-2
[16] Aguilera-Alonso D, Alonso-Cadenas JA, Roguera-Sopena M, Lorusso N, Miguel LGS, Calvo C. Monkeypox virus infections in children in Spain during the first months of the 2022 outbreak. Lancet Child Adolesc Health. 2022;6(11):e22-e23. doi:10.1016/S2352-4642(22)00250-4
[17] Ladhani SN, Aiano F, Edwards DS, et al. Very low risk of monkeypox among staff and students after exposure to a confirmed case in educational settings, England, May to July 2022. Euro Surveill.2022;27(40). doi:10.2807/1560-7917.ES.2022.27.40.2200734
[18] Vusirikala A, Charles H, Balasegaram S, et al. Epidemiology of Early Monkeypox Virus Transmission in Sexual Networks of Gay and Bisexual Men, England, 2022. Emerg Infect Dis. 2022;28(10):2082-2086. doi:10.3201/eid2810.220960
[19] Hennessee I, Shelus V, McArdle CE, et al. Epidemiologic and Clinical Features of Children and Adolescents Aged <18 Years with Monkeypox — United States, May 17–September 24, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(44):1407-1411. doi:10.15585/mmwr.mm7144a4
Thanks very much for the recognition about my tweets. I was so enraged that these people were leveraging their doctorates to such ill effect. These doctors clearly didn't know what they were talking about, clearly didn't do the homework by reading up on the epidemiology, and clearly had a problem with expressing any concern for the very real suffering that gay men were enduring last summer. Instead, they wanted to spread harmful fear and hysteria that kids were all going to get the virus at daycare. I can't tell you how many messages I got from parents who had been needlessly frightened, wondering if they could safely send their kid back to school in the fall. It is tragic but unsurprising to learn that despite tweeting with no basis in actual science, these scientists won the misinformation war.
I'm especially proud of the work I did on Twitter (all my reporting on mpox is here: http://www.benryan.net/mpox.html), because at the peak of the misinformation wave, I was very ill with side effects from the chemo I was undergoing for cancer at the time (I was cured). The chemo made me pretty manic, so I found that my brain rhythms synced nicely with the frenetic energy of Twitter. As burdened as I was medically, I found that fighting this fight took me away from my own woes.
Also, FYI, here's a greatest hits thread I did of the worst mpox misinformation: https://twitter.com/benryanwriter/status/1607503033318916096?s=20
This paper has demonstrated what many of us MD MPHs who follow the evidence based data have been saying: these “experts” are not experts at all.