
Semi-automated offsides technology and diagnostic expansion medicine
Can we learn from the World Cup?

If you are enjoying the World Cup, you will have seen the use of semi-automated offsides technology.

Using multiple cameras and digital 3-d reconstruction, offsides can be called when as little as 1 mm of a player has advanced past the defender. Offsides has long been a rule in soccer, but these days the enforcement is rigid.
Some soccer fans don’t like the new 3-d enforcement. They argue that this technology has changed the spirit of the game. Specifically, it has removed the “attacking nature” of soccer. Because players can be disqualified for the smallest offsides position, they are more tame, reluctant to leap at a scoring opportunity.
Offsides is a simple, unchanging rule, but it is different when it is performed in real time with flags, when it is reviewed on videotape, and when it is determined by automated digital reconstruction systems. It raises the question of whether or not all offsides is the same? Can a difference in degree become a difference in kind?
Of course the analogy could not be more apt for medicine. We all know what a stroke is, a cerebral perfusion defect and symptoms. But what is a stroke in the era of extremely sensitive MRI machines? Sometimes patients are flagged for having a stroke who have no neurologic deficits.
We all know what a blood clot in the leg is, but is it different if you present a painful calf versus if you're asymptomatic and it is found on screening ultrasound?
Is it still the same afib if you find it with your apple watch? In one trial, 14 day screening found more afib, lead to more anticoagulation, but there was no difference in stroke. Apple watch trials are ongoing.
And with cancer, is all metastatic disease the same? We have widespread stage migration.
Even the endpoint in our clinical studies is not exactly what we see in the clinic. Every doctor knows what shingles is. It's bad. The endpoint of the randomized controlled trial of Shingrix is not exactly shingles. It is detection of the virus after this happens:
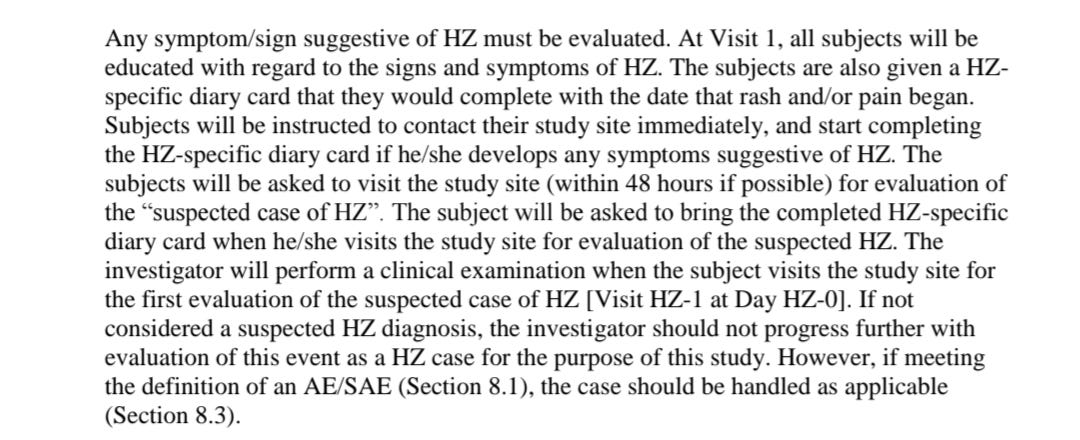
Is there a difference between shingles when the patient, untrained in Shingles, notices something is wrong and seeks the care of the doctor versus shingles when the patient is educated to be vigilant for shingles, keeps a diary about shingles, and contacts the doctor for anything that may or may not be shingles with a hair trigger?
Is there a difference between being offsides when it's visible to the sidelines referee and the flag is in the air, and semi-automatic offsides detection technology that finds your elbow is past the defender?
Soccer purists say it changes the attacking spirit, and similarly, using diagnostic categories that bend with technology may alter the therapeutic benefit of interventions— finding disease that doesn’t need treatment— or creating a false perception of the benefit of a therapy— exaggerating the value of a preventive by averting pauci-symptomatic disease that would not have been diagnosed without a course in detection.
The idea that technology can change a rule, not by definition, but by the margin of detection, is a lesson both soccer fans and doctors should appreciate.
I agree (and to my surprise similar technology has also metastasized to baseball!) This philosophy should instead be applied to enhance critical appraisal so that journals and editorials become more selective to high quality studies.
So, like purified water still has coliforms, the touted disease free periods in oncology are misnomers? Birds Eye view vs satellite imagery. Mammograms with CAD vs without. Our technology advances and resets the ranges, remember never use the word “ normal “, making it more challenging to interpret and categorize whats happening because we all want black and white only, greys need not apply.