
The Hubris of Screening for Disease -- Again
JAMA has published an eye-opening analysis of colorectal screening in Veterans. Why doctors cannot see the obvious message continues to surprise me

One thing you learn from years of working in the hospital is the utter unfairness of disease. You see people doing everything right—diet and exercise—and still succumb to some often obscure noncardiac cause of death.
There are thousands of fatal diseases that can take you out. It doesn’t even have to be disease; a car wreck can be fatal. This fact has always made me see screening for disease in asymptomatic people as foolish. In other words, even if a screening test had perfect sensitivity and specificity it would still fail to prolong life.
A recent observational study of more than 90,000 US veterans’ only strengthens this take. The specific study question obscures the larger message of competing causes of death—AKA other shit that can kill you.
The Study
The UCSD-led team focused on the risk of colorectal cancer (CRC) and all-cause mortality in people age 75 years or older who had (or did not have) an adenoma on a previous colonoscopy. Current guidelines recommend stopping screening colonoscopy at age 75, but what if the patient at age 72 had an adenoma?
[Quick background: adenomas are polyps — abnormal growths projecting from the mucosal lining of the colon or rectum that have undergone dysplastic (pre-cancerous) changes. They matter because colorectal cancer almost universally follows the adenoma → carcinoma sequence. This process takes years.]
Using the VA database the authors made two groups of patients: those with and without an adenoma on colonoscopy before age 75. The main outcome measures were the incidence of CRC, CRC death and non-CRC death and all-cause death.
Of the 91,000 patients (mean age 71), 28% had an adenoma and 72% did not have one.
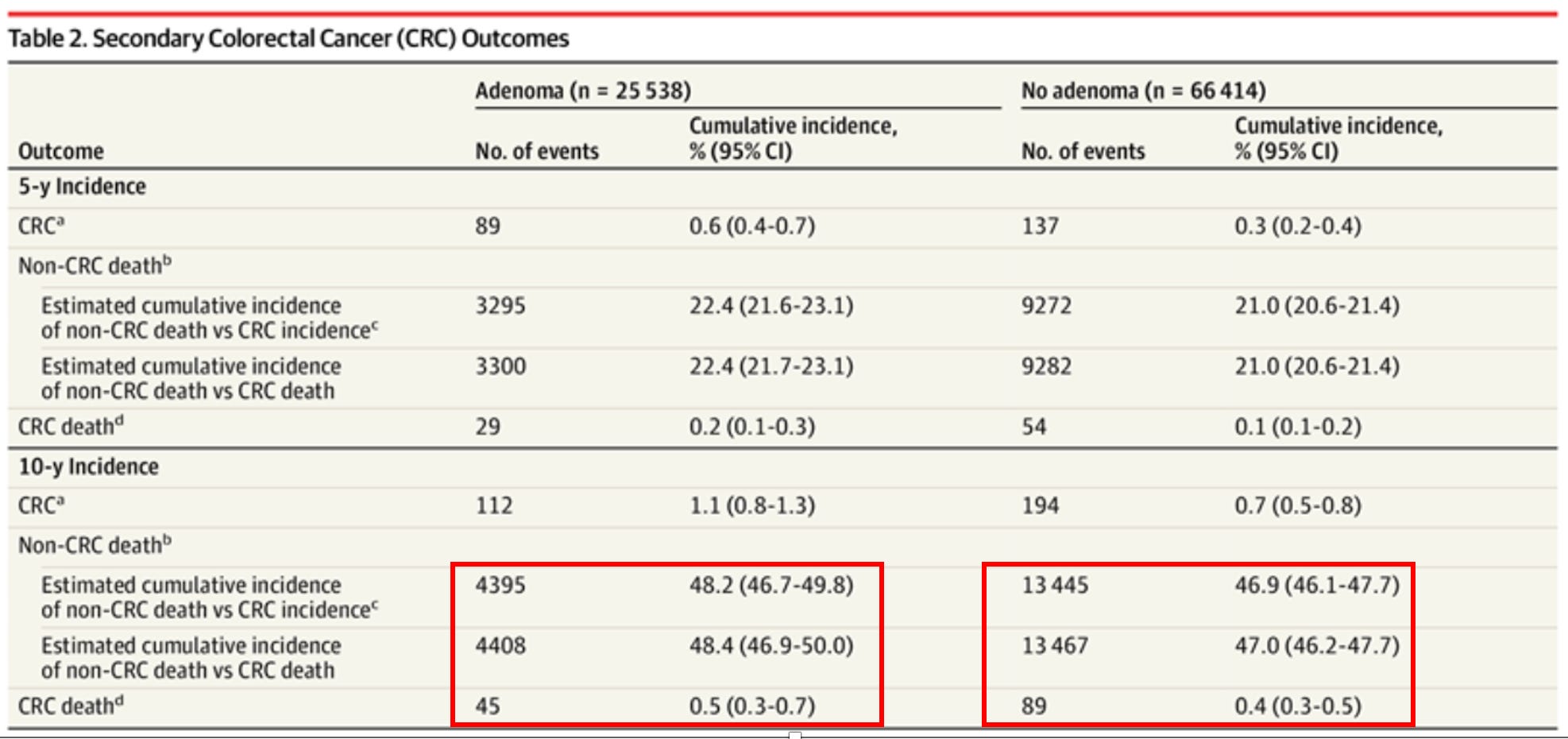
At 10-year follow-up, the cumulative incidence of CRC was 1.1% in those with adenoma vs 0.7% in those without adenoma.
At 10-year follow-up, the cumulative incidence of CRC death was 0.5% in those with adenoma vs 0.4% in those without adenoma.
The cumulative incidence of non-CRC death ranged from 46.9% to 48.4% at 10 years.
I’ve attached a screenshot from the paper. Look at the red rectangles. In the 25,000 pts with adenomas before age 75, there were 45 patients who died of colorectal cancer over the next decade. But there were 4,408 patients who died of something else.
Many of you may ask about higher risk adenomas. There was no difference in future cumulative CRC risk.
Comments
The authors spend a lot of gentle words in their discussion explaining how it is reasonable to stop doing colonoscopy after age 75—even when there is an adenoma.
I would look at the larger picture.
From the Table above, the 10-year risk of dying from colorectal cancer at age 71 (the average age of this study) was 0.5% even if you had an adenoma. The risk of dying from something other than colon cancer was 48%.
Now do fractions: 48% divided by 0.5% = you are 96 times more likely to die of something else. Not 50% higher; not double the risk, but 96 times more likely.
This study was done in 71-year-olds and we all know that death comes to us all, and the older we get, the higher the odds of all diseases. So a screening advocate might argue that we should keep screening but do it in younger people.
My rebuttal would be what do you think the ratio of CRC death to other death looks like at age 60 or age 50 years?
Well… we can look at the NordICC trial of screening colonoscopy published in NEJM in 2022.
In the 56,000 individuals in the control arm of that study, 157 people died of colorectal cancer (0.31% over 10-years) vs 6079 people who died of any cause (11%). Younger people therefore only have a 36x greater risk of dying from non-colorectal cancer. (By the way, the ratio was the same in the screening arm: 11% vs 0.28%).
Bottom Line:
If you have blood from the rectum, or a strong family history of colon cancer, you should be checked.
But if you are a regular person, how does it make sense to look for one disease when you are 36-90 times more likely to die from something else. I am asking. Tell me.
It remains obvious that the human mind cannot rationally integrate the meaning of statistics for the most part. This is something we need to examine and determine on a societal basis. If we spend inordinate amounts of dollars on the health of 80+ year olds - even when we have good evidence that the testing we are doing is not changing anything re: longevity - we have less resources to focus on younger people. It is clear that both physicians and their patients have personal bias ingrained that is difficult to overcome. Add to that the extreme arm-twisting message we've given patients (and physicians) for the past 20 years: all driven by quality metrics that force physicians to make sure all their patients have said screenings done (the voracity with which we've chased and admonished people to get their <mammogram, colonoscopy, blood testing> have given all of us the sense that you'd be unwise not to comply - in fact, it makes us all very uneasy if patients don't agree to do their screenings).
So now, as a society, we are dealing with the fallout of the age of Quality Metrics arm-twisting. People (and physicians) will not just change their mind and see things in a more rational and measured manner.
We need public health to make some firm guidelines that should be followed. Patients should be given clearly written statements re: pros/cons of the available screening tests and their potential risk for developing these conditions. they can ask their physician for input if needed. And follow guidelines that make sense on the larger scale. Patients then make up their own mind on what makes sense to them, within the general guidelines.
It is a waste of physician time to talk a 94 year old woman out of doing a mammogram. Why do I need to do that?
I find it unsettling that we have let our society evolve to a point where young people don't want to have children for the sake of "overpopulation" and climate change, where not all of them know their blood pressure or their blood sugars as they may not have health insurance or the time to go see a doctor, yet we want to make sure the 80+ year olds are perpetually screened and studied: even when there is clear evidence this is not helpful. Makes you go "hmmmm"...
And points out a major negative consequence of "Quality Metrics" in the first place. Who'd a thought?
The recent data from JAMA on the results from the WISDOM study in breast cancer also echoes- this using mammogram to screen all women for breast cancer does not show mortality benefit in the way that risk based mainly genetics and family history screening does. But between clinical guidelines emphasizing population health and hospital economics incentivizing screening (all covered under the ACA, guaranteed payment), it's going to take a long time to track towards risk-based screening.