
The inertia of clinical trials and unethical control arms
An example from Multiple Myeloma teaches an ethical lesson in oncology

It is my pleasure to introduce this guest column by Manni Mohyuddin MD. The piece discusses a topic near and dear to my heart. The control arms of cancer trials.
I always tell fellows, a trial can only change your practice if the control arm is your practice. Yet sadly many trials use outdated controls. The same investigators who insist we adopt the latest drugs are happy to participate in global randomized trials where control arm patients get outdated, inappropriate, and suboptimal care. In 2018, Derrick Tao (now MDAnderson Fellow) and I wrote about this in the Lancet Onc.

In 2019, Talal Hilal (Now Faculty at Mayo Scottsdale) documented that 1 in 5 trials sent for US FDA approval used a control arm that was beneath the US standard, and I discuss this at length in Malignant book.
But what sense does this make? How can we approve a drug for use in the US when we don’t know it is better than what we are already doing in the US?
Ironically, these global trials help neither the citizens of the US nor global nations. The moment the trial begins it is uninformative in the US, and the moment it ends the drug is unaffordable globally. Instead it is part of the predatory practice of modern oncology.
In the guest post, Manni Mohyuddin from Huntsman Cancer Institute discusses a recent example of this problem, and his emotions on the topic. If you enjoy his essay, learn more in Manni’s recent paper.

Vinay Prasad MD
The inertia of clinical trials and unethical control arms
Manni Mohyuddin
I started fellowship firmly believing in the mantra the best treatment for a patient with cancer is a clinical trial. Indeed- for the cancer I specialize in- multiple myeloma, there have been tremendous breakthrough discoveries, which have been tested rigorously in clinical trials and have led to dramatic improvements in survival. Yet, as I learnt through my fellowship, there are also some examples of trials that are unethical and flawed, with control arms that were highly unfair.
Over the last several decades, a complex system of bureaucracy has evolved to protect patients enrolled on clinical trials. These include institutional review boards, federal regulations/oversight, and countless other processes. Unfortunately, though, as we will learn, the time involved in these processes, coupled with the pharmaceutical industry’s ambition to have their product succeed at (almost) all costs can result in some clinical trials being deeply flawed and far worse than standard of care for patients enrolled on them.
Myeloma is a cancer that currently can be controlled for prolonged periods of time, but generally not cured. Using high dose chemotherapy followed using one’s own stem cells to help the blood counts recover (autologous transplant) is a standard treatment for myeloma. Yet, this procedure is not curative- and patients need some sort of ongoing treatment afterwards (maintenance) to keep disease under control.
The first trial showing that a drug called lenalidomide when used as maintenance improved “overall survival” was published in the New England Journal of Medicine in May 2012. Yet because some other trials showed that lenalidomide improved the time alive without cancer progression (progression free survival) but not overall survival, uptake of lenalidomide was not universal until several years later. Nevertheless, at the American Society of Clinical Oncology Meeting in June 2016, a patient level meta-analysis (compilation of data from multiple trials) was presented showing that lenalidomide maintenance improved overall survival in multiple myeloma. The writing was on the wall and the data clear.
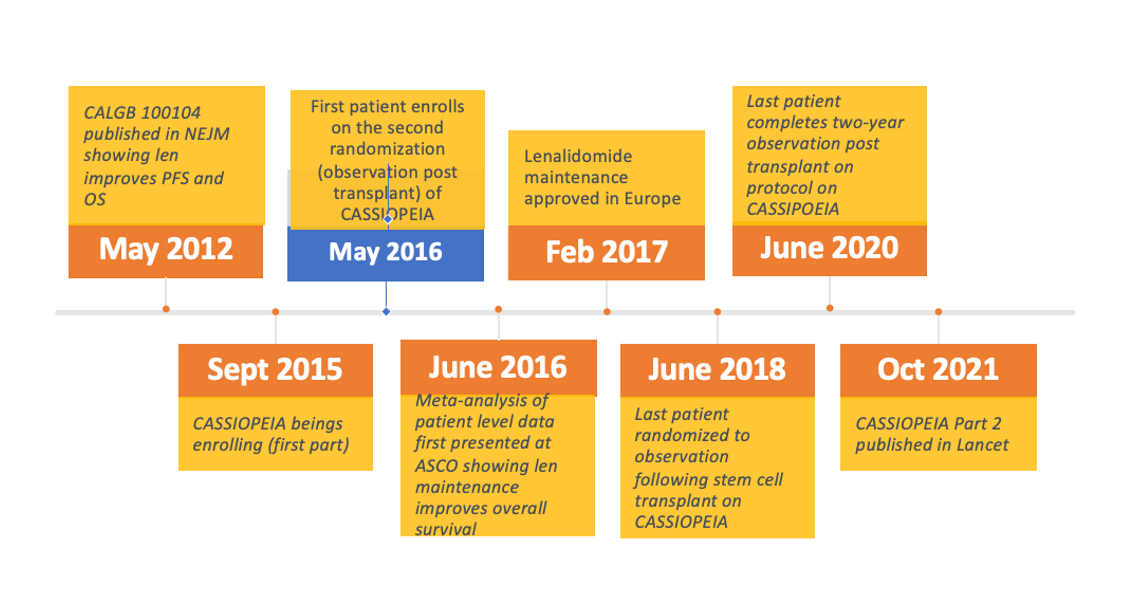
Figure 1: Timeline of this trial and lenalidomide maintenance
Enter now a new trial called the CASSIOPEIA trial enrolling in Europe, which randomized patients to either observation without therapy or a drug called daratumumab as maintenance after transplant. The endpoint (what this trial was statistically powered to show) of this part of the trial was progression free survival (PFS).
The trial first enrolled a patient September 2015, although the randomization to maintenance with daratumumab versus observation did not happen until May 2016. Now, I would argue to you that for the endpoint that this trial was designed to show improvement in (PFS), we already knew that lenalidomide was better than observation, before a single patient was enrolled. I concede however that uptake of lenalidomide may not have been universal (especially so in Europe) in September 2015.
Nevertheless, by June 2016, one month after the first patient was randomized to observation, it was abundantly clear that patients on observation after stem cell transplant lived shorter compared to those on lenalidomide maintenance. By Feb 2017, lenalidomide was approved in Europe as maintenance post-transplant. However, this trial continued to enroll and randomize patients to observation. The last patient on this trial was randomized to observation June 2018. The observation period lasted at least two years (in absence of frank disease progression) according to the protocol, and hence the last patient would have been continued to formally observed off treatment in June 2020, eight years after the “first trial” showed lenalidomide was effective in this situation, four years after a meta-analysis showed unequivocally that patients lived longer with lenalidomide maintenance, and over three years after lenalidomide was approved in Europe for this purpose. If this is not a moral tragedy of the inertia of our trial designs and regulatory oversight, then I do not know what it is. As they say, an image speaks louder than a thousand words and Figure 1 highlights the timeline of this process.
Every single employee of the company that ran this trial (Janssen) that I have personally met has been delightful, conscientious, and firmly committed to making the world a better place. The doctors/trialists who ran this trial are all those I tremendously respect who overall have made life tremendously better for the thousands of people diagnosed with myeloma every year. Yet, if we do not recognize this as a flaw and disservice to the patients on the control arm, we are destined to repeat the same mistakes.
Why was the system not nimbler? Why did the protocol not change? There were years of opportunities where this could have been done. I recognize that I was not part of the discussions during the process. Perhaps Janssen tried to change this, and the regulatory authorities did not let this happen? Perhaps the regulatory authorities felt that a midway change to the trial would render the findings of the trial useless. However, I offer to you one simple question. Did the patients on the control arm clearly know that they were sacrificing (potentially) years of their lives just so that the trial could continue in its current fashion? Perhaps it was for the greater good that the trial continue in its current fashion so that a quick and clean answer was provided and daratumumab be approved for thousands of people in Europe. If that was the case though, those patients should have clearly known that they sacrificed for the greater good.
I write this with the best of intentions, with complete awareness of my ignorance of some of the processes involved. It is a complex multifactorial process, and there are thousands of conscientious people who are more experienced than me involved in every step of the way. I also have never practiced in Europe and may not be aware of the situation there (although I am from Pakistan originally and know a little bit about different healthcare settings, having recently seen my dad’s ischemic stroke mismanaged back home). I do not want to impose my American standards on another country, but I’d like to think access to a life prolonging medication is within the reach of a large pharmaceutical industry running a trial. Even if local regulatory authorities had not approved lenalidomide during the period this trial ran, Janssen could have amended the trial and provided the drug to the control arm (there is now law stopping an ethical company from providing access and going “above” local regulatory standards). And there is precedence- a recent acute lymphoblastic leukemia trial was amended midway when new data came out regarding the efficacy of blinatumomab. Why couldn’t our field do the same?
I leave you with more questions than answers. But if we continue to rationalize and make excuses for why this happened, we are destined to repeat the same mistakes. For the sake of our patients who sacrifice so much to be on these trials, let us do better. Let us advocate for more nimble protocols, more advocacy for all patients (even if they are in other countries on control arms of regulatory trials), more patient-facing trials, and regulatory oversight that hastens rather than impairs growth.
 | A guest post by
|
Thank you Dr. Mohyuddin for your insight on this challenging, complex and important subject. Having spent the last year fighting myeloma we have learned that the patient and family needs to do significant reading, thinking and consulting on decisions around clinical trials. While they are important in advancing our knowledge, to do so at the expense of the patient seems unethical. You are a true patient advocate.
I was taught that a trial is only ethical if it is *unknown* which arm would have the better outcome. Was there no data safety monitoring board on the CASSIOPEIA trial? Or does outside data, showing the trial is no longer ethical because which arm has better outcomes is now known, not fall under their bailiwick? Does true informed consent, a notion that seems to be almost a distant memory, as it was intended, not extend to updated information during a trial, when there is new information pertinent to a subject's informed decision to remain in the study or not? We do have to guard against situations like those that happened with AZT and the COVID injections, though, where the trials were stopped, blind broken, and placebo/comparator arm given active intervention after only a very short period, since there's no way to know about longer-term adverse events than to have a placebo/comparator arm.