
The Most Ignored Study in Cardiac Electrophysiology
The Study of the Week explores the DANISH trial -- a major study that is largely ignored

In days of old, we placed implantable cardioverter–defibrillators (ICD) in patients who survived cardiac arrest. The problem was that survival of out-of-hospital cardiac arrest was terrible.
Smart people then designed studies to place ICDs in patients before they had cardiac arrest. We call this primary prevention. You can’t place ICDs in everyone because the device comes with downsides (infection, inappropriate shocks, anxiety and costs, for instance.)
One of the main drivers of cardiac arrest is a weak heart muscle, so-called heart failure. Patients with low-ejection fraction despite medical therapy are said to be “eligible” for an ICD.
The Big ICD Trials
The first big trial, MADIT 2, enrolled patients with HF due to previous heart attack. We call this ischemic cardiomyopathy. MADIT 2 was a success. The ICD reduced death by 5.6% in absolute terms and 31% in relative terms.
Heart failure, though, can occur via non-ischemic means. Non-ischemic cardiomyopathy confers a slightly lower risk of cardiac arrest compared with ischemic CM.
The DEFINITE trial enrolled only patients with non-ischemic causes of HF. In this case, the ICD reduced overall death by 35%, but it did not reach statistical significance. The technical interpretation of the trial was that it was null. The reason for lack of statistical significance was a low number of events (*note: non-ischemic HF has a lower arrthymic risk than ischemic HF).
One year later, NEJM published the results of the SCD-HeFT trial, which randomized more than 2500 patients with both non-ischemic and ischemic HF to amiodarone, placebo or an ICD. The overall results favored the ICD. The relative risk reduction from the ICD was 23% but the absolute risk reduction was a whopping 7%. That’s an NNT of about 14.
The issue for non-ischemic HF patients came in the subgroup analysis. While the ICD provided a statistically significant reduction in death in patients with ischemic disease, the ICD failed to meet statistical significance in non-ischemic patients. See slide.

This is strange.
Thus far, there had been no single trial with non-ischemic HF in which the ICD showed clear benefit. The first lesson I think is that for an ICD to provide benefits>harms, there has to be a high enough baseline risk of cardiac arrest.
Now to a stranger thing: the ICD retained a Class 1 indication despite the less-than-strong evidence. You might wonder how that happened.
The Power of Clever Meta-Analyses
Four authors from Harvard published a meta-analysis of five studies that they purported to study ICDs in non-ischemic HF patients.
Boom. When you combine the studies, the ICD effect becomes positive. But there is a twist.
The study with the largest effect was called Companion. But it was not a simple ICD trial. It included a special kind of ICD, one with biventricular pacing. Don’t get hung up on the details. Suffice to say, Companion did not belong in the meta-analysis.

The DANISH Trial
I was there when Professor Lars Kober presented the results. DANISH enrolled 1100 patients with non-ischemic HF. They followed these patients for nearly 6 years. They only enrolled sick patients (median ejection fraction 25%) but they insisted on appropriate medical care of heart failure.
Here were the results:

No difference in death rates at six years.
The one caveat from DANISH was the possibility of something we call heterogenous treatment effects. Or HTE. Younger patients may have derived an ICD benefit, whereas older patients may have had harm.
I hesitate to show the subgroup analysis because trials are powered for main results. Look, for instance, at how few patients there are in the younger category. Subgroup analyses are always at risk of seeing noise more than signal.

Comments
I am not against ICDs. I implant ICDs. But there is clearly a difference in risk between non-ischemic and ischemic heart failure. In 2024, we now subdivide non-ischemic HF into many groups, but we have no studies regarding ICD benefit/harms in these subgroups.
There is also a bit of an expiration date issue.
When the early ICD trials came out positive, background medical therapy was not as good. Primary PCI was less available than it is now.
Over time, heart failure therapy has improved. And. As background therapy improves, the rate of cardiac arrest falls. This reduces the benefit of an ICD.
HF trialists have actually published a study showing this.

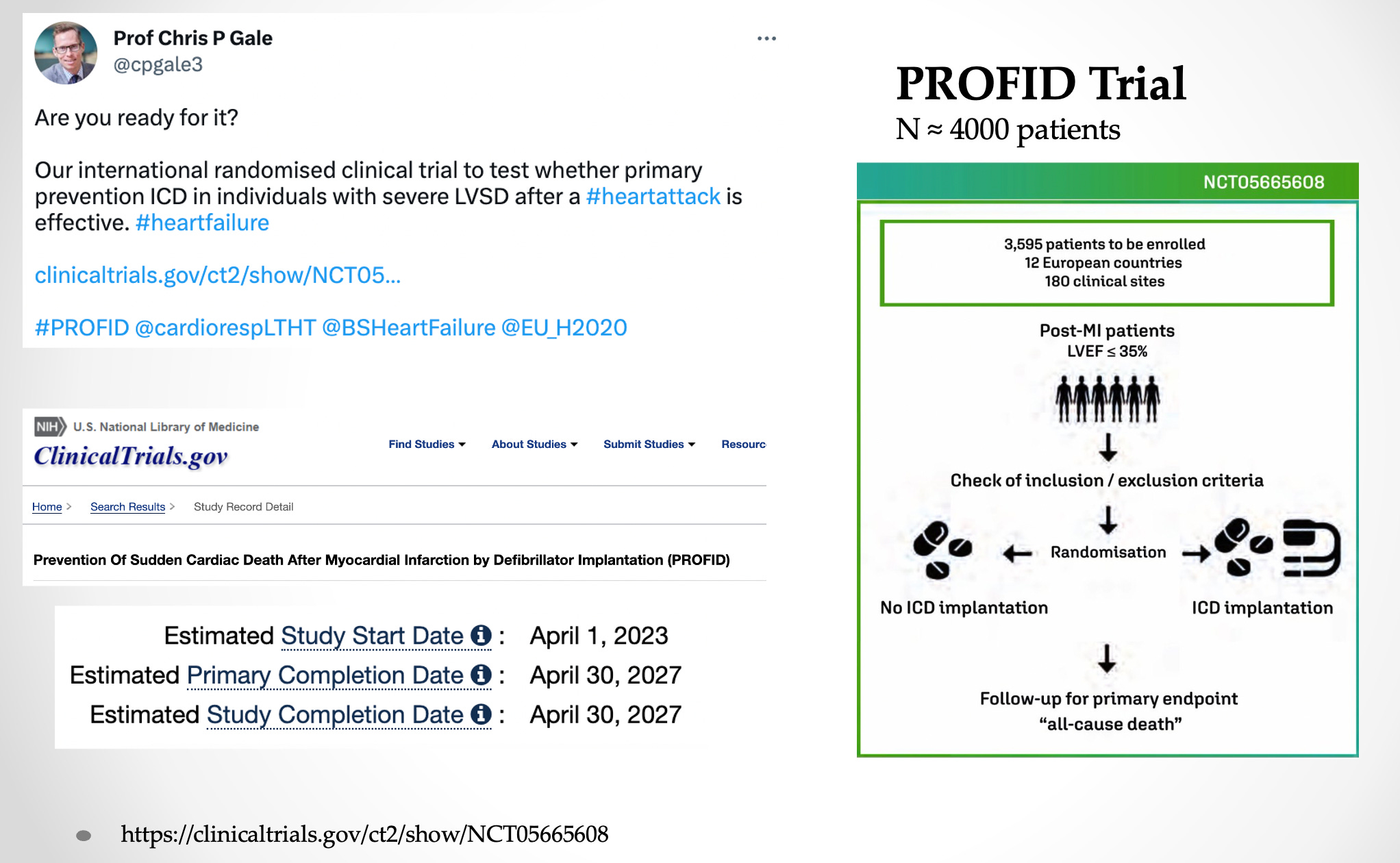
Lower rates of ventricular arrhythmias is likely the reason DANISH did not find an ICD benefit. Now, brave investigators from Europe will repeat the first big ICD trial (MADIT 2).
The PROFID trial will enroll patients with ischemic cardiomyopathy to ICD or medical therapy. This is bold. And it requires a European mindset. PROFID could never happen in the US, because American doctors think less with their science brains than do Europeans.
Get this
It is now 8 years past DANISH trial. Guidelines still do not incorporate DANISH and the previous slew of studies showing no ICD benefit in non-ischemic patients.

Before DANISH, there was little supportive data for the ICD in non-ischemic causes of heart failure. Then DANISH comes out non-significant. There are clear declining temporal trends in sudden cardiac arrhythmias and improving medical therapy of heart failure.
Yet our experts still give an ICD the highest possible recommendation.
Let me know what you think. I am perplexed. JMM
You won’t say the obvious, doctor, so I will.
My first ICD cost $28,000 (not including the surgeon’s fees, hospital charges, and associated medical expenses). That was in 2004. I get a new model every five years, plus I am monitored remotely at home and away. This is a big business — and only the most naive readers will ignore the monetary incentive of implanting unnecessary ICDs in patients with good insurance.
My own personal experience with an ICD was a living nightmare. My mother survived cardiac arrest at age 58 but had only had 75% of her heart muscle left and was living with an EF of less than 35% for several years. So they implanted an ICD in her at age 75, telling her that this would save her if she had another cardiac arrest. She did have another one at age 86. The ICD shocked her over 25 times as her heart kept stopping and that little device was determined to keep her heart going. An ambulance quickly took her to the hospital where they had to intubate her to keep her breathing. Her blood pressure plummeted so they gave her 3 different medications to prop it up. I had medical power of attorney but not knowing what her true condition was I wanted them to keep her going. After she had been days in the ICU and still unable to breathe on her own, the cardiologist told me that he knew she only had 10% of her heart muscle left and would never breathe on her own again. It would have been nice if he had shared that with everyone else. After that, I had the job of telling my mother and asking her permission to turn off all the interventions that were keeping her alive, including that ICD. So the ICD had restarted her heart, but to what purpose? The damage to her heart was done. I find it hard to believe that this result is not happening time and again with these devices. The cost? Over $80k, all paid by insurance. But this was several years ago, I shudder to think what it would be now. Again and again I am reminded of that saying from Jurassic Park, “your scientists were so preoccupied with whether or not they could, they didn't stop to think if they should.”