
The Problem of Incidental Coronary Artery Calcium on a CT Scan
Finding incidental CAC has become common. A recent guideline document says this is heart disease and should be treated with meds. Let's assess this strong statement.

Social media was abuzz with discussion over the new lipid management guidelines that came out last week.
You would not think treatment of abnormal lipids would be that complicated.
Yet the document spans 134 pages, 14 treatment flow charts, 45 brand-new recommendations and 8 revised recommendations from the last guideline in 2018. Most controversial was the large number of class 1 recommendations—26 of 53.
Today we call out the class 1 recommendation on the matter of incidental coronary artery calcium (CAC) on a CT scan done for something else.
What is a Class 1 Recommendation?
This is the highest form of a recommendation. It means “should be done” or “is indicated/effective/beneficial.” In the upper right corner of the image below is a benefit greater than risk with 3 greater than signs.
Examples of class 1 recommendations in other areas of cardiology include ACE-I in heart failure, anticoagulation in patients with atrial fibrillation and risk factors and urgent stenting for patients with MI.
Class 1 recommendations often morph into quality measures, which reward (or penalize) doctors and systems for following or not following a guideline. Class 1 recommendations can become known as “standard of care.” And failure to follow standard of care can lead to malpractice liability.
In nearly every other guideline document, Class 1 recommendations usually stem from the strongest evidence. Often multiple randomized controlled trials. Guideline writers grade the level or quality of evidence behind a recommendation with levels A (multiple RCTs), B-R (1 RCT), B-NR (nonrandomized observational studies), C-LD (limited observational or mechanistic studies) and C-EO (expert opinion).
Incidental CAC
Here’s an image of the class 1 recommendation for incidental CAC
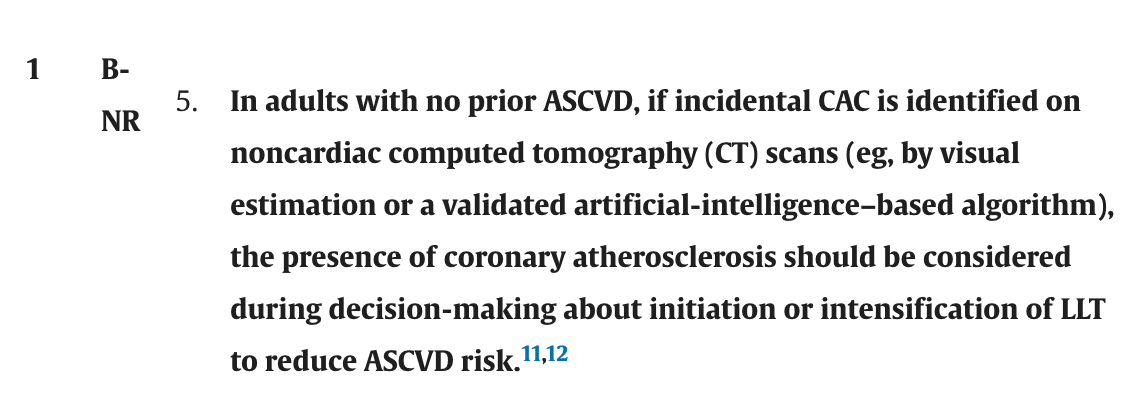
The writers say that CAC indicates coronary artery disease, which puts the person into the category of secondary prevention where lipid lowering therapy is indicated.
Since it’s class 1, you’d expect that there are multiple trials suggesting lipid lowering therapy improves outcomes in patients with incidental CAC. But there are not.
Note the blue numbers above. One references a single-center observational study that associates incidental CAC to worse outcomes compared with no-CAC. As the authors write in their limitations, this study is susceptible to bias. The other reference goes to a study associating carotid plaque to incidental CAC. That is it. Two references and one does not pertain to the issue.
Comments
This is just one example of overestimation of evidence in the guideline document. I will have more to say about other parts of the guideline. As a teaser, I counted only 10 of 46 class 1 recommendations have the highest level (A) evidence.
I chose this one example because a) incidental CAC is increasingly common due to the huge numbers of people getting CT scans, b) the utter lack of trial-level evidence for a class 1 indication and c) the potential consequences of having this as a class 1 recommendation.
Let me expand on the consequences: a urologist orders a CT scan for a kidney stone. In addition to a large stone, the radiologist notes incidental CAC. The patient is 75 years-old. A year later he presents with a massive MI and dies. The family could easily sue the urologist for not starting a statin for the incidental CAC.
That scenario may sound far-fetched, but consider the sheer number of different clinicians ordering CT scans. You can get a CT scan before even seeing a doctor in an ER waiting room.
The recommendation to treat patients with incidental CAC with lipid-lowering drugs has almost no evidence. One single-center observational study is cited.
While it makes some sense to assume this is coronary artery disease and treat, any reader of Sensible Medicine knows how scary it can be to base doing things in Medicine that make sense.
What’s more, I would ask how many of these patients with incidental CAC would be indicated for lipid-lowering therapy on the basis of the pooled cohort equation? I bet most.
If I were writing this document I would have put incidental CAC in areas of uncertainty and made no recommendation. Or, at most, made it a Class 2b, level of evidence expert opinion.
I don’t understand the urge to make recommendations in the absence of evidence. Why not just say nothing when there is no evidence? The document had more than 25 academic peer reviewers. How does this not get called out?
A very welcome post about this issue! We're making people sick and overmedicated. I usually say to my patients: "keep exercising, enjoy life, eat helathy food, sleep and stay away from doctors".
Wondering:
1). What percent of the population (over the age of 75) DO NOT have CAC?
2). Why the big rush to treat everyone (past the age of 10) with a statin?