
"Toxic" quizzing: Is the attending mean or is the resident sensitive?
Facts can be adjudicated; tone is challenging

Recently, I read an article on “toxic” quizzing. It’s was about attendings asking trainees questions in a mean way.

Does it happen?
Yes, of course. When I was a medical student, there was only one drug approved for HER-2 positive breast cancer. It was traztuzumab (this was before lapatinib). A breast surgeon, known for pimping, asked me about it in the OR.
VP note: My story is true
Attg: What is the name for the small molecule inhibitor this patient will get after surgery?
Me: Hmmmm, I don’t know. There is no small molecule inhibitor approved that I am aware of. There is one in trials, nearing approval, I think.
Attg: Oooooh, so, so sorry, it’s traztuzumab. I am surprised you don’t know that.
Me: But uhh, traztuzumab is a monoclonal antibody.
Attg: Yes, a small molecule.
Me: (trying to resist the urge, and muster a neutral tone) Hmmm, but monoclonal antibodies are like the molecular size of a Buick, not really small, right?
She didn’t give me a good evaluation.
To me, she was not only condescending, but she didn’t know what she was talking about. And in that respect, she was in good company.
17 years later, I realize that there were many incorrect things I was pimped about in my training. Often with an asshole/ dickish tone of voice, but sometimes with a kind voice. I was often pimped incorrectly, but nicely.
Atenolol is a great first medication to start for hypertension.
Of course, all combinations happen. The attending is wrong, and an asshole (the breast surgeon). The attending is right, but an asshole. The attending is wrong, but nice (atenolol). The attending is right, but nice.
Here is the challenge. It’s easy to referee if the factoid is correct. But who decides if the attending is nice or not? You heard the story the way I remember it. Is my memory correct?
Recently, I saw this on X, where the trainee does not dispute she did not know the answer, but focuses on the tone: it was, to her, meant to embarrass.
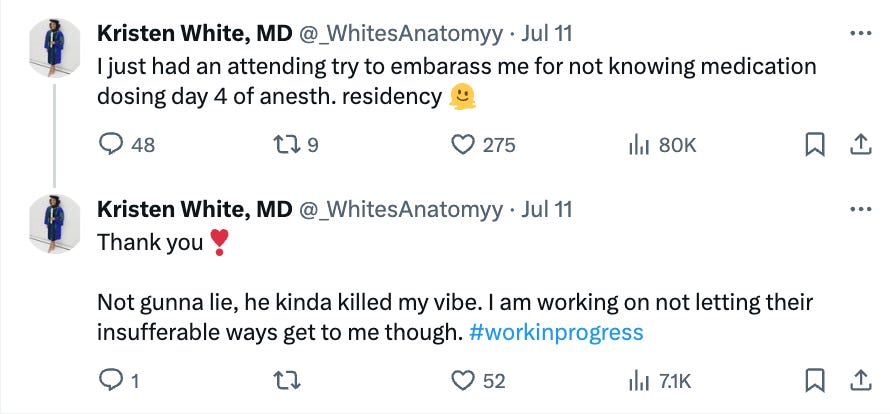
One commenter asks the key q:
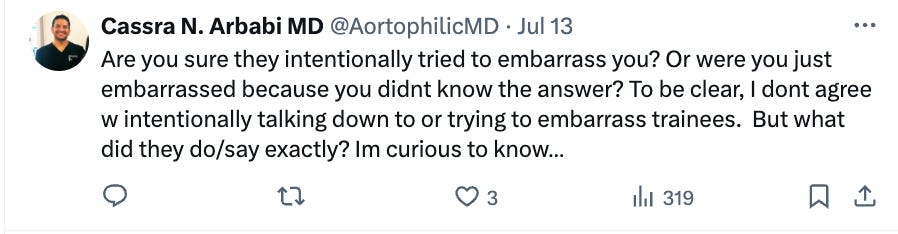
What exactly did the attending do and say? That’s the tough question. And who heard it? What was their mood and perception? Were there bystanders? What if the stories differ?
VP’s note: What follows is my imagination of an investigation. It is pure fiction meant to illustrate a point
If I were investigating this as a detective would— I would interview the parties.
First, the attending.
I asked her what dose of Versed we should give, and she didn’t know. I suggested she take a look at page 20 of the resident handbook before tomorrow. It has doses of all the common meds. Then I told her the dose.
Then I interview the resident
This was an unplanned procedure, or I would have read about it beforehand. Dr. Jones asked me what dose of Versed I wanted to give. I said I didn’t know. Then he said I should probably read more before each case. Had I known this would be today’s case I would have read it! Also, he said it in front of the whole team. I found his comment insulting and meant to embarrass.
Then I interview the NP on the team.
Dr Jones asked Dr. White what dose of Versed she wanted to give. She said she didn’t know. He suggested that, as a general rule, she should prepare for cases, and that page 20 of the resident handbook would be a great starting point, and cover most situations she will encounter. Then he told her the dose.
Then I interview the med student on the team:
Dr. Jones asked me what dose of I think Ativan— I wanted to give, I said, I don’t know. Then he asked Dr. White, she said she didn’t know either. Then he told both of us that page 20 of the resident handbook has all the common doses, and later after the case, he gave me a copy and an extra copy to give to Dr. White in case she lost hers, and also because its nice to have a copy at work and home.
At the end of my investigation, I would conclude, I have no fucking clue if the tone used was appropriate or not. I would also wonder what I did wrong in this life to have to investigate things like this.
Thus the challenge: is the attending mean or is the resident sensitive?
In my opinion, since I started medical school, I believe attendings have become nicer, and trainees have become more sensitive. But the biggest change is the administration. They are now capitulate blindly to trainees. An attending who makes a comment that is perceived as mean even if it is not can easily be banned from working with students or fired. The net result is that we lose attendings who push trainees and we fill our ranks with medical educators who are nice. Sadly, whether or not anyone is saying anything true is largely un-adjudicated.
Without any information many online commenters know that the resident’s story is *correct*.

I don’t know how we can solve the issue of “toxic” questioning because ultimately it often boils down to she said/ he said. Some cases are egregious, but most will be gray. There isn’t the bandwidth to prosecute these cases.
Ultimately, my concern is that administrators are going to do whatever minimizes complaints which means attendings will be demoted, or incentivized to say nothing at all and whether or not residents are getting the best training and education will remain an afterthought.
Authors note: I also read this tweet which fueled my imagination.

Dr Prasad has been prolific in pointing out how the making of doctors as an endeavor is failing, just as all other institutions that have embraced DEI and WOKE ideology
Once Drs lost their autonomy, where Attendings have to worry about student-trainee evaluations rather than making sure they taught the material and set a good example all was lost
Most older doctors will tell you that there was no official with whom to lodge such a trivial complaint. We would tell our war stories to one another. There were Attendings who struck fear into trainees, they were usually the most brilliant , talented ones. The Attendings that were known to produce the best results in their patients were usually the most demanding of excellence in their students, who then jockeyed to become their residents Those Attendings drove themselves as hard a# they drove their trainees. The bureaucracy simply did not exist for nonsense.
Back in the day, when all IV bottles were glass, OR drapes were cloth and 20-bed open wards were the norm, it was not unusual to be interrogated with questions such as "Why is tape white?" or " Would you rather have a transcaphoid perilunate dislocation or a transtyloid transcaphoid perilunate dislocation?" It happened to all of us. We commiserated, shrugged it off, and accepted it. It built resilience for the morbidity/mortality conferences. I can recall times when fellow residents were emotionally abused, which is never to be condoned, but the toxic quizzing was just a rite of passage.