
Tricuspid Valve Interventions and its Dubious Evidence
The Study of the Week revisits the lessons of VPS I and VPS II to show the failures of tricuspid valve intervention trials

I have a great (and sad) story to tell today. It’s about hubris and the need for proper control arms in device trials.
The reason control arms popped in my head was an unusually candid editorial in JAMA regarding the management of tricuspid regurgitation.

The authors criticize the evidence base underpinning the new push to intervene on the tricuspid valve. I wrote about the fatally flawed TRILUMINATE trial here on Sensible Medicine in 2023.
The JAMA editorial is strong, but it is too late. Tricuspid regurgitation may be the most common valve condition; it’s present in almost every patient with heart failure, but it is almost never the primary problem.
No matter, enthusiasts now have multiple percutaneous tools (a clipping device called transcatheter edge-to-edge repair) and a completely new valve (called the EVOQUE). The short story is we are on the brink of a massive increase in tricuspid valve procedures.
The problem is simple and obvious: the positive trials (TRILUMINATE and EVOQUE) supporting these transcatheter procedures were driven only by subjective quality of life measures. There was no reduction in death or hospitalizations. While QOL is an important endpoint, it is utterly biased when there is no placebo control. In an intervention vs med trial there will surely be a strong placebo effect.
Now let me show a glaring example of why proper controls are needed. I was in my third year of private practice when excitement ensued about using pacemakers to treat patients who had vasovagal syncope.
Most of you have seen vasovagal syncope. Often in church, or in an operating room, a standing person develops low blood pressure and low heart rate, and if they don’t lie down, they faint. Once supine, the heart fills with venous return from the legs and the vagal response stops. On a tilt table test, some patients can have profound bradycardia. Like 20 seconds of asystole.
The VPS 1 Trial
JACC published the paper in 1999.
The trial procedure line sounded innocuous. “Patients with ≥6 lifetime episodes of syncope and with a tilt-table test that induced syncope or presyncope, as well as a relative bradycardia, were randomized to receive a dual-chamber pacemaker or not.”
The primary outcome was unbiased: the first occurrence of syncope. Trialists planned to enroll 284 patients but after a pilot study of 60 patients, the effect size was so big, they stopped enrolling.
Here was the result
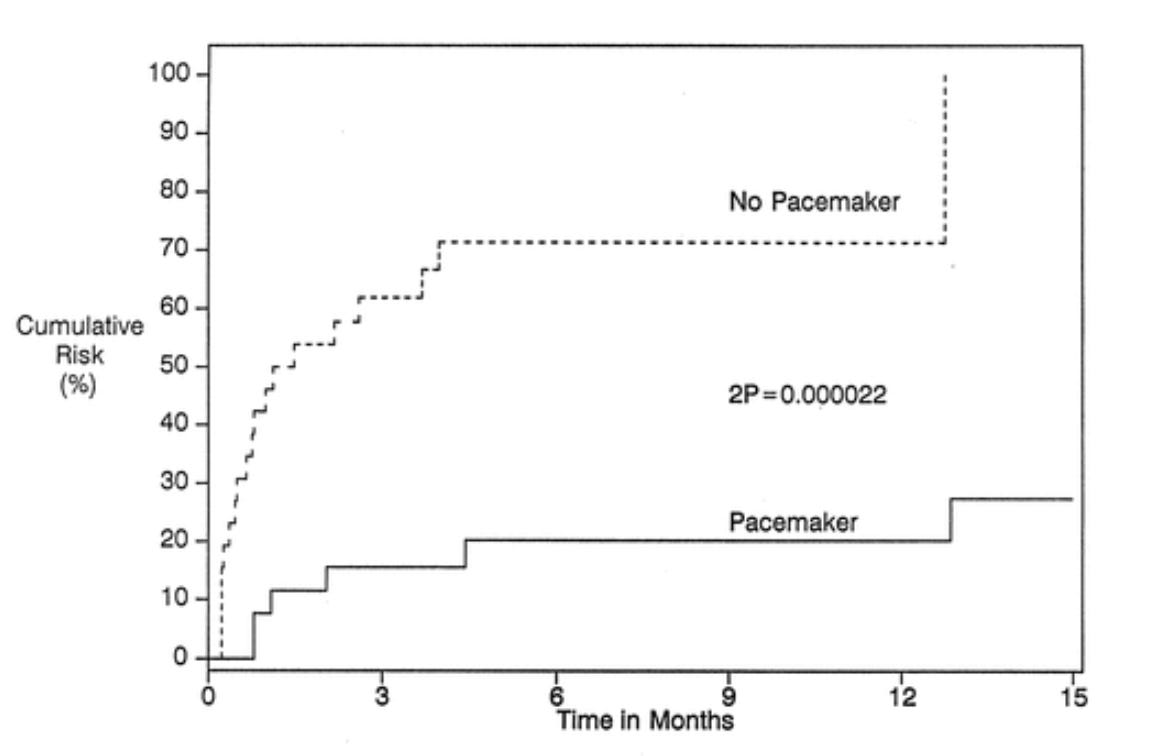
A massive reduction in syncope. The conclusion read that dual-chamber pacing reduces the likelihood of syncope in patients with recurrent vasovagal syncope.
The authors explained in the manuscript that pacing works by treating the bradycardia. They did however note the possibility of bias due to the unblinded nature of the trial. They even wrote in the discussion:
A study in which all patients receive a pacemaker with subsequent blinded randomization to pacemaker on or pacemaker off would provide even stronger evidence that pacemaker therapy helps these patients.
The VPS II Trial
That is exactly what the same Canadian team did. In VPS II, published in JAMA in 2003, all 100 patients with multiple episodes of vasovagal syncope and bradycardia, received a pacemaker. One group had pacing turned on, the control arm had the pacer turned off.
Here were the results:

Pacing complications occurred in 7 patients.
The conclusions were the opposite: pacing did not reduce the risk of recurrent syncope and because of the weak evidence of efficacy of pacemaker therapy and the risk of complications, pacemaker therapy should not be recommended as first-line therapy.
Comments:
I show the VPS 1 and 2 trials to illustrate the importance of trial procedures and the need for proper control arms when studying outcomes in device trials.
We must now cite the important Faith Healing and Subtraction Anxiety paper by Christopher Rajkumar and the team at Imperial College London.

Without such a placebo (or sham arm in device trials), patients in the control arm may suffer from subtraction anxiety. While patients in the device arm feel “faith healed.” That is, they believe they will be better; they may also do other things to avoid a bad outcome. Vasovagal syncope can be modifiable. Patients in the pacing arm may have avoided situations that induce syncope.
In VPS II, all patients had the pacemaker. None knew their treatment assignment. And the results show no significant difference. This result totally reversed the 1999 VPS I trial.
Young doctors may not know why pacing therapy should be avoided in young people with vasovagal syncope. But the lesson of VPS I and II transcend one condition.
The lesson is that you need a placebo control when studying outcomes in device trials.
The TR device trials omitted a proper control arm. They used the methods of VPS 1. FDA regulators allowed it.
I called the tricuspid regurgitation trials a failure of regulatory oversight, but David Cohen rightly corrected me, writing that there was plenty of blame to spread around.

The thing is that tricuspid valve interventions will become commonplace. Money will be spent, patients operated on, and we will not know if there is benefit. The TR intervention trialists completely ignored the lessons of VPS I and II. All that it would have taken is a simple sham tricuspid valve arm.
I am not sure why this happens. I hope the new leadership at FDA will bring more rigor to the regulatory process. But Dr. Cohen is correct, the investigators should know better. These are scientists who are well versed in evidentiary methods. I wonder what was said in the trial planning process.
I am sad because stuff like this shreds trust in medical science.
I think most responsibility for this problem lies with the FDA. If the FDA allows a lower standard of evidence, the device companies will insist on designing pivotal trials to meet it. The concerns of physician PIs will not be able to overcome these economic forces.
Retired surgeon here. We are taught early on in training how to read and decipher papers. Along with having to do studies/ papers also to try and get published. Can't help but think the physicians doing that tricuspid valve study know better but did it anyway. Infuriating