


Universal Depression Screening Leads to Unnecessary Harm
Twenty two years since the USPSTF’s original depression screening guidelines, the practice is still not supported by evidence

Regardless of the reason for a primary care visit in the United States, patients are routinely asked how often they feel “hopeless” or "like a failure”. These questions come from the PHQ-9. The PHQ-9 has since been validated and is now widely used to screen for depression. Since the United States Preventive Services Task Force (USPSTF) first recommended depression screening 22 years ago, the practice has become standard in primary care despite an absence of evidence.
The adoption of depression screening is, of course, well-intentioned. The harder we look for depression, the more people we can try to help. With depression and anxiety diagnoses on the rise, screening seems the sensible thing to do.
But I’ve learned that screening can lead to a cascade of interventions more likely to harm than help.
USPSTF Guidelines
Depression screening was first recommended to adults in 2002 with a “B” grade. Seven years later, in 2009, the USPSTF expanded this guideline to include children as young as 12 years old. At this point, the USPSTF admitted this recommendation was based on “no studies [that] evaluated the direct benefits of screening compared with no screening or usual care”.
With the bar for evidence lowered, the USPSTF accelerated the publication of similar guidelines. In October 2022, the USPSTF recommended childhood anxiety screening starting at eight years old. In June 2023, the same was recommended to adults. For both recommendations, the USPSTF found "no studies that directly evaluated the benefits of screening for anxiety disorders."
Regardless, the USPSTF concludes there is “moderate certainty that screening for anxiety… has a moderate net benefit”, the rationale for a “B” grade.
Since the beginning, these recommendations have drawn criticism. A 2008 Cochrane review found adult depression screening does not improve outcomes. A subsequent article in BMC Medicine highlighted the dearth of evidence. The title of this article kind of says it all:

The authors suggest a depression screening RCT should exclude individuals with known depression, randomize people to screening or no screening, and make the same mental health services available to both groups. Sounds reasonable.
I might add that the mental health services in the study should be those actually available in the population being studied.
The USPSTF claims "screening interventions" decrease the prevalence of depression at six-month follow-up by an odds ratio of 0.60. This number is surprising when we consider the following:
A meta-analysis of six RCTs found the benefit of SSRIs, compared to placebo, to be small and statistically insignificant at six months.
Cognitive behavioral therapy decreases depression rates (OR 0.64) and the benefit appears to be more durable than pharmacotherapy. But in the real world, not everyone who screens positive for depression ends up in therapy.
So where did these numbers come from?
In an “Evidence Synthesis”, the USPSTF cites three statistically significant RCTs. All of them are postpartum screening trials. The first appears convincing, but the findings are invalidated by the fact that primary and secondary measures were changed post-hoc and depression symptoms improved far beyond what is expected.
In the second cited trial, weekly at-home counseling was provided to the screening arm, but not the control arm. In the third trial, an unspecified number of patients in the “control” arm were, in fact, screened for depression. Again, the intervention and control arms received different support services.
The last two trials convincingly demonstrate that when patients with postpartum depression have better access to mental health services, outcomes improve.
None of these trials adequately test or quantify the benefit of postpartum depression screening, not to mention universal depression screening. The USPSTF claims direct evidence is unlikely to be generated, given screening is now the “standard of care”.
While relying on a flawed evidence base, the USPSTF did not cite more applicable trials.
In a 2017 Lancet trial, 10,190 personnel from the UK military were randomized to post-deployment depression screening or no screening. Similar mental health services were available to both groups. Screening had no impact on depression, anxiety, or a host of other mental health outcomes.
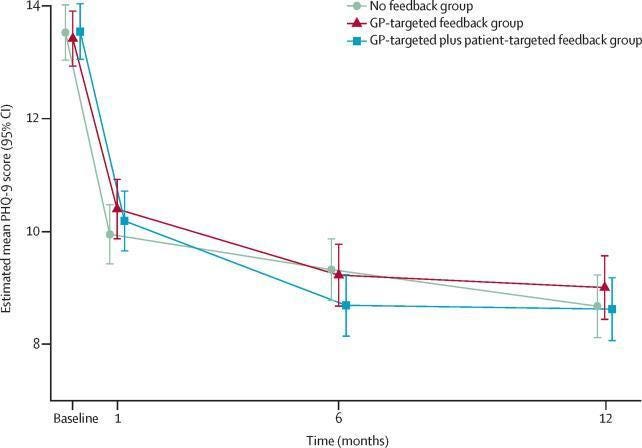
Outside the United States, it seems understood that depression screening doesn’t lead to better outcomes. Another Lancet trial, this one from Germany, screened patients with the PHQ-9 but randomly dictated what happened with the results. The results were shown to the general practitioner and patient, only the general practitioner, or to nobody. PHQ-9 scores tended to improve regardless.
Uncertainties
Misdiagnosis
Misdiagnosis is common with screening. Medical illness, other psychiatric illness, and life circumstances can lead to positive results on the PHQ-9. The PHQ-9 is known to overestimate the true prevalence of depression by a factor of 2 (24.6% vs 12.1%).
Ineffective treatment
Whether or not depression screening takes place, the graph above shows that remission is the most likely outcome. This result can be explained in a number of ways:
Those who benefit from depression treatment are detected without screening.
Mild depression – depression that would only be detected by screening – tends to resolve without intervention.
The benefit of screening is just too small to be detected by well-designed trials.
Treatment Harms
Screening exposes patients to harm from overdiagnosis. Treatment with antidepressants, whether appropriate or inappropriate, carries risk. The FDA recently approved escitalopram for pediatric generalized anxiety disorder based on an 8-week trial that found the medication increased suicidal ideation 6.5-fold (NNH=14, p=0.01).
Off Target Effects
Primary care physicians are overwhelmed. Adding one more box to the endless “to do list”, a box whose tick may not help the patient, is bad for the doctor and all his or her patients.
The onus is on the USPSTF, and other advocates of depression screening, to demonstrate a net benefit from screening in the real world. No trials adequately weigh the harms and benefits of anxiety or depression screening in the United States.
A Case
I got interested in this topic because of a patient.
Sarah, as I will call her, came to the clinic for a school physical. I became fixated on her screening PHQ-9 score. She ended up on antidepressants.
With each follow-up appointment, I learned more and more about Sarah. She is brilliant, well-read, and excels in school. After COVID lockdowns, she struggled to readjust to in-person schooling.
After six months of taking antidepressants, Sarah ended up in an emergency room. She had overdosed on her antidepressants.
Fortunately, she was discharged the next morning. She didn’t intend to harm herself. Rather, she felt the antidepressants were not working anymore. She thought taking more medicine might help.
We agreed to leave the pills behind. In retrospect, we should have done so sooner. Perhaps my decision-making was flawed from the start. Her mental health improved as she learned to navigate the mad world around her. She joined a school club related to her interests and made good friends. On subsequent visits, she possessed an aura of confidence I had not seen before.
She found her way despite my heavy-handed management.
Wil Ward is a PGY-3 family medicine resident at West Suburban Medical Center in Oak Park, IL. Upon graduating, he plans to practice in Iowa and continue writing on his own Substack.
Photo by Anthony Tran
 | A guest post by
|
It seems there is a pill for every ill. It was refreshing to hear you admit medication had not been a good treatment for your patient Sarah. Sometimes a person just needs to do something different like join a club or something. We all get depressed sometimes but meds should be a last resort imo. Thanks for posting! Sabrinalabow.substack.com
Thank you for this. Every year my former GP went through this exercise and would offer me antidepressants. I gave an honest answer as I care for my husband and have been involved in care for my elderly parents for over 15 years. Who wouldn’t be depressed. However I have never taken the medications and from what I see others have simply floundered with side effects and more complications than the depression alone when using these meds. I understand psychiatry as I have a family member with mental illness but medications are not the be all end all for depression. More often it is the need for a good social network and exercise that gets one going again.