
Vaccine analyses in nonsensible times

By Christine Stabell Benn, Frederik Schaltz-Buchholzer, Sebastian Nielsen, and Peter Aaby, Bandim Health Project, University of Southern Denmark and Guinea-Bissau
Many thanks to Sensible Medicine for publishing the guest post by Charlotte Strøm entitled “The False Narrative of Nonspecific Vaccine Effects”.
In times where vaccines are increasingly politicized, any researcher whose research nuances the message about vaccines beyond “safe and effective” must anticipate being heavily criticized. As researchers studying the overall health effects of vaccines for many years, we are familiar with this reality.
Strøm sets out to contradict the existence of nonspecific vaccine effects (NSEs). This concept that was defined by the Bandim Health Project, starting with Peter Aaby’s discovery of strongly beneficial effects on all-cause mortality of measles vaccine in Guinea-Bissau in the 1980s. These beneficial effects were so pronounced (a ~70% reduction in all-cause mortality) even though there were no measles deaths because there had been a measles epidemic the previous year. This suggested that measles vaccine could induce broad protection against pathogens that might otherwise have killed children. We coined the effects “non-specific effects”. The findings were confirmed elsewhere, and the discovery of beneficial NSEs is now recognized as one of Nature’s “Milestones in Vaccines”.
Since then, the authors of this article and other researchers have been investigating NSEs for other vaccines. All the vaccines studied – mainly in low-income settings with high child mortality - have shown evidence of NSEs. The pattern observed is that live-attenuated vaccines like measles vaccine and BCG vaccine (against tuberculosis) have beneficial NSEs. More worryingly, non-live vaccines like diphtheria-tetanus-whole cell-pertussis vaccine (DTP*) may be associated with increased female mortality. The NSEs are most pronounced while a given vaccine is the most recently administered, making the sequence and combination of vaccines very important.
Though these findings were initially met with skepticism, epidemiological studies in combination with immunological studies have convincingly shown that vaccines affect the broader innate immune system, leading to wider acceptance of NSEs. The World Health Organization (WHO) reviewed the evidence for NSEs of measles vaccine, BCG and DTP vaccine in 2016 and concluded that “(…) receipt of BCG and MCV reduce overall mortality by more than would be expected through their effects on the diseases they prevent, and receipt of DTP may be associated with an increase in all cause mortality (…)” The latest edition of the World’s leading text book in vaccinology “Plotkin’s Vaccines” has a whole chapter devoted to NSEs. It is thus somewhat belated for Charlotte Strøm to claim that NSEs are a “false narrative”.
DTP vaccine
Strøm is particularly concerned with the potential negative NSEs of the DTP vaccine on female mortality. So are we. DTP is one of the world’s most widely used vaccines, recommended in low-income settings as a primary series of three doses in infancy (typically around 6, 10 and 14 weeks of age). Furthermore, many countries recommend a 4th DTP vaccine (a “DTP-booster”) around 18 months of age.
It is unfortunately not possible to conduct randomized trials of the primary DTP-series as it is not possible to give the first DTP earlier than 6 weeks and it is ethically problematic to delay it. Hence, our research into the NSEs of DTP has relied on natural experiments and observational studies.
Our main observations, along with those of other researchers regarding DTP vaccine are as follows:
First, DTP vaccine protects against the target diseases and there is inherent healthy vaccinee bias in all observational studies, so in such studies, the DTP-vaccinated children should have slightly lower mortality than the DTP-unvaccinated children, if DTP has no non-specific effects. This is what is seen for other vaccines. Thus, any relative risk increase in DTP-vaccinated vs. DTP-unvaccinated children is a signal that DTP has negative NSEs. Therefore, it is worrying that prospective studies without survival bias comparing DTP-vaccinated and unvaccinated children have consistently found increased mortality following DTP-vaccination (Figure 1).
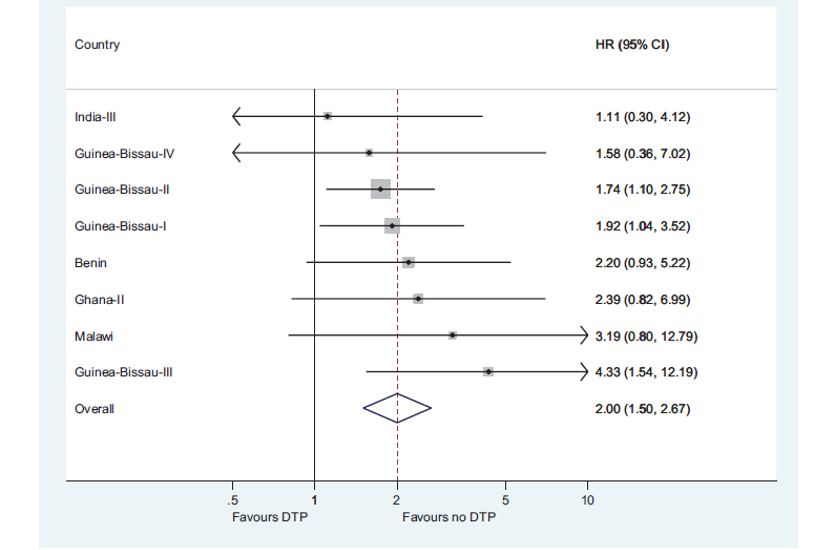
Figure 1. The mortality rate ratio for DTP-vaccinated versus DTP-unvaccinated children in studies with no survival bias. From Aaby et al, Pediatr Infect Dis J 2016.
Second, nearly all studies of DTP indicate that DTP is associated with higher female-than-male mortality. In the pre-vaccination era, girls had slightly lower mortality than boys, at least in West Africa. So, the pattern depicted in Figure 2 of increased female-to-male mortality is unusual and concerning.
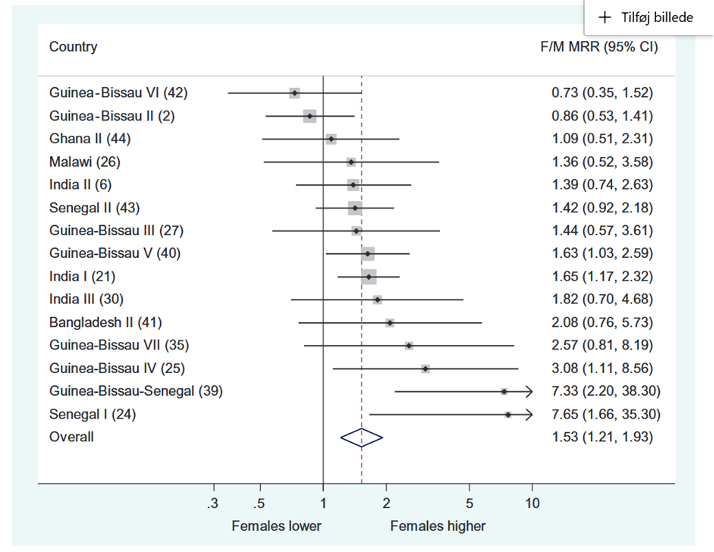
Figure 2. Female/male mortality rate ratios among DTP-vaccinated children. F/M: female/male; MRR: mortality rate ratio. From Aaby et al, Trans R Soc Trop Med Hyg. 2016.
Third, in all studies where DTP’s impact is examined along with the impact of BCG and/or MV, using the same epidemiological methods, DTP is associated with a more negative effect than BCG and the measles vaccine (Figure 3).

Figure 3. The mortality rate ratios for BCG-vaccinated versus BCG-unvaccinated, DTP-vaccinated versus DTP-unvaccinated and measles-vaccinated versus measles-unvaccinated children in the 10 studies with no or limited survival bias. From Aaby et al, Pediatr Infect Dis J 2016.
Fourth, the WHO had to withdraw a new high-titer measles vaccine (HTMV) because it was repeatedly associated with increased female mortality. It turned out that the explanation was that HTMV had been given so early that most children received DTP after the HTMV. The increased female mortality was only seen in HTMV recipients who received DTP after HTMV.
All these findings point to a problem: increased female mortality after DTP vaccine.
No NSEs of DTP vaccine?
Strøm’s “claim to fame” – and the two main points covered in her post – centers on her review of DTP for the Danish Medical Journal (in Danish), in which she states that she found no evidence of NSEs, and that she has “discovered” an unpublished study of DTP vaccine by our group.
Let us deal with these two points one by one.
Strøm admits that she is not a researcher, nor a vaccine expert. That is unfortunately quite evident from her review, which suffers from significant errors and should not have passed peer-review. We have critiqued Strøm’s review here (in Danish).
In brief, she omits substantial portions of the literature, misreads or miscites wrongly some studies, and makes basic errors such as confusing female-to-male mortality ratios with male-to-female mortality ratios.
In her attempt to miscredit us Strøm quotes a previous employee wrongly and without permission, resulting in an erratum from the journal.
In her Sensible Medicine article Strøm repeats errors from the Danish review. E.g., she writes “Further, the Bandim group was unable to replicate their own findings, when the hypothesis – that the DTP vaccine as a non-live vaccine is killing children – was revisited in 2018”. The study she refers to concludes that “In the three studies of the introduction of DTP in rural and urban Guinea-Bissau, DTP-vaccinated children had an HR of 2.14 (1.42-3.23) compared to DTP-unvaccinated children; this effect was separately significant for girls [HR = 2.60 (1.57-4.32)]”. It should be evident to most that this is a clear confirmation of the hypothesis.
Strøm particularly criticizes a DTP study mentioned by Secretary Kennedy. She neglected to mention that this is a natural experiment, which is as close to a randomized trial as one can come. We have previously addressed Kennedy’s reference to our trial in a LinkedIn article, where we go through the literature on DTP, and explain that while some details were inaccurate, the overall message - that we discovered a serious safety signal in relation to DTP vaccine for females - is correct.
Unpublished study
Strøm accuses us for not publishing a DTP trial while simultaneously calling for more DTP trials. Strøm’s lack of familiarity with the vaccine research is also evident here. The trial in question examined the DTP-booster at 18 months of age, comparing a 4th dose of DTP versus not receiving a 4th dose. Thus, all children had received at least three DTP vaccines. This is obviously a different study from the studies of the primary DTP vaccine series, comparing DTP-vaccinated children with DTP-unvaccinated children, which have been the focus of our quest into the overall health effects of DTP-vaccine (including the study mentioned by Kennedy).
The unpublished study was disrupted by force majeure, including positive events (a pregnancy of the PI) and negative events (a death of the local supervisor), as well as structural challenges (during the trial period, Guinea-Bissau changed vaccination policy in several related areas and had many interfering national vaccination campaigns). Furthermore, mortality during the trial period dropped to just 20% of the anticipated rate, rendering the trial underpowered to address the mortality effect of the 4th DTP vaccine. We have laid out the crude mortality data which shows that the trial is inconclusive (being compatible with both large benefits and large harms of the 4th dose of DTP vaccine). Of course, the study should still be published, and we are working on that. But it should be clear that this study, underpowered and studying a different subject, is not going to contradict the findings of increased female mortality after the primary DTP-vaccine series.
Conclusion
In times of polarized views on vaccines, attacks are expected if one presents nuanced data on vaccines. We have soberly reported on our findings on the overall health effects of vaccines. We have found incredibly beneficial effects of some (live) vaccines, and less positive, even harmful, effects for females of other (non-live) vaccines. This has resulted in us being tagged “antivax” as well as “pharma-bitches”.
We are open to data that contradict our conclusions. As we navigate the evolving understanding of non-specific effects, we are also consistently testing our own findings – occasionally we contradict ourselves, which we consider fortunate as it signals something we have not fully understood yet.
Unjustified and unsubstantiated criticism from individuals like Strøm, who offer no data but simply try to discredit our publications, is merely a nuisance. Strøm has a company that works for the industry. On the website of her company Sharpen, she describes that she offers advice to “pharmaceutical, biotech and medical technology companies”. We can only speculate about her motives for devoting so much time going through our studies of negative NSEs of vaccines.
Nothing in Strøm’s article justifies her assertion of a “False Narrative of Nonspecific Vaccine Effects”. Robust epidemiological and immunological evidence supports the existence of NSEs. While the safety signal in relation to female mortality after DTP vaccine (and other non-live vaccines) is a significant and worrying concern, the overriding message is that the discovery of NSEs hold great promise for improving the overall health impact of vaccines by optimizing both their specific and their non-specific effects.
* Note that DTP is a different vaccine from the diphtheria-tetanus-acellular-pertussis vaccine (DTaP) used in high-income settings and from the pentavalent vaccine (that in addition to DTP also contains vaccines against H. Influenzae type b and hepatitis B) currently used in many low-income settings.
 | A guest post by
|
Vaccines are becoming like a religion. Criticizing them is like denying the resurrection. The fanatics who think they have an obligation to suppress all vaccine criticism are the ones creating vaccine hesitancy, not the RFKs. People know that RFK is just one guy with an opinion. But in a world where no one is allowed to look for problems with a medical treatment, they will never be found – even when they exist. This attitude is breaking trust in vaccines.
"It is unfortunately not possible to conduct randomized trials of the primary DTP-series as it is not possible to give the first DTP earlier than 6 weeks and it is ethically problematic to delay it. "
Ethically problematic is the same circular reasoning behind using other vaccines as the "placebo" in the RCTs for licensing. You assume that the risks of the disease are higher than the vaccine, which is the very thing the RCT needs to prove. The only reason i can see to do this is to cover up the safety concerns with the vaccine being tested.