
Vaping: The Great Innovation Public Health Failed to Embrace
Part II: Why Public Health Has Been Opposed

In part I of Dr. Satel’s articles on vaping, she reviewed the facts about vaping and its use. Today, in part 2, she will address the politics of vaping and the roots of opposition.
Adam Cifu, MD
In the State of the Union address this month, President Biden revived his "Cancer Moonshot" initiative. First introduced during the Obama Administration, the President hopes the campaign succeeds in cutting the cancer death rate in half over the next 25 years.
Because cigarette smoke is a potent carcinogen, every tool should be used to decrease cigarette smoking. E-cigarettes should be one of these tools but, as I discussed several weeks ago, many public agencies refuse to recognize them as a vehicle that can help get us to the moon.
Given that vaping is undeniably less hazardous than smoking, that e-cigarettes have helped millions quit smoking, and fears that e-cigarettes would "re-normalize" smoking among adults and lead teens to take up smoking have not materialized –in fact, smoking is at historic lows in the U.S. – why the resistance to vaping?
When e-cigarettes were promoted as a safer alternative to smoking, tobacco-control advocates immediately recalled the public health disaster of the “safer cigarette,” unveiled by tobacco companies in the late 1960s. These cigarettes were not safer. The cigarettes included ventilated filters, small holes in the filter that were intended to introduce air and thereby dilute the smoke inhaled. But smokers reflexively covered the holes with their lips or fingers, defeating this effect. Smokers also took more puffs, longer puffs, or more vigorous puffs to compensate for low-tar cigarettes’ weaker taste.
By the late 1980s, the tobacco-control movement had become opponents of “safer” products, maintaining that the tobacco industry could not be trusted. And they were right, a point illustrated at the infamous 1994 congressional hearing that further exposed their deception. During this hearing, top executives of seven major tobacco companies asserted, in tandem, that “nicotine is not addictive.” The next month, 4,000 pages of internal industry documents from a leading tobacco company spanning four decades were leaked and eventually published in 1996. The papers confirmed that the company had been aware of the cancerous effects of smoking for decades but continued to maintain that "causation has not been proved."
Thus, when e-cigarettes came to the market in 2006, tobacco control advocates were hostile to the notion that any product was safer — the very term "harm reduction" became synonymous with industry deception — and were distressed by the very optics of e-cigarettes smokers exhaling large plumes of vapor. The critics were especially concerned since vaping devices delivered nicotine in a satisfying manner, with enjoyable flavors.
"Many saw in e-cigarettes a Trojan horse that would slow the process of smoking denormalization, reduce the number of people trying to quit, and seduce young nonsmokers," wrote Amy Fairchild and colleagues in the New England Journal of Medicine in 2018.
The CDC also adopted the stance that vaping was just a smoke-screen for another nicotine delivery system."Guilty until proven innocent," is how then-director Dr. Thomas Frieden spoke of e-cigarettes in 2013.
I would argue that healthy skepticism is one thing, but a failure to promote the benefits for adult smokers because of a worry about the effects on youth was, and is, misguided.
The Surgeon General, in his 2016 report, and the 2018 National Academies of Sciences, Engineering and Medicine report on e-cigarettes, both asserted that nicotine vaping was a ‘gateway’ to smoking for young people.
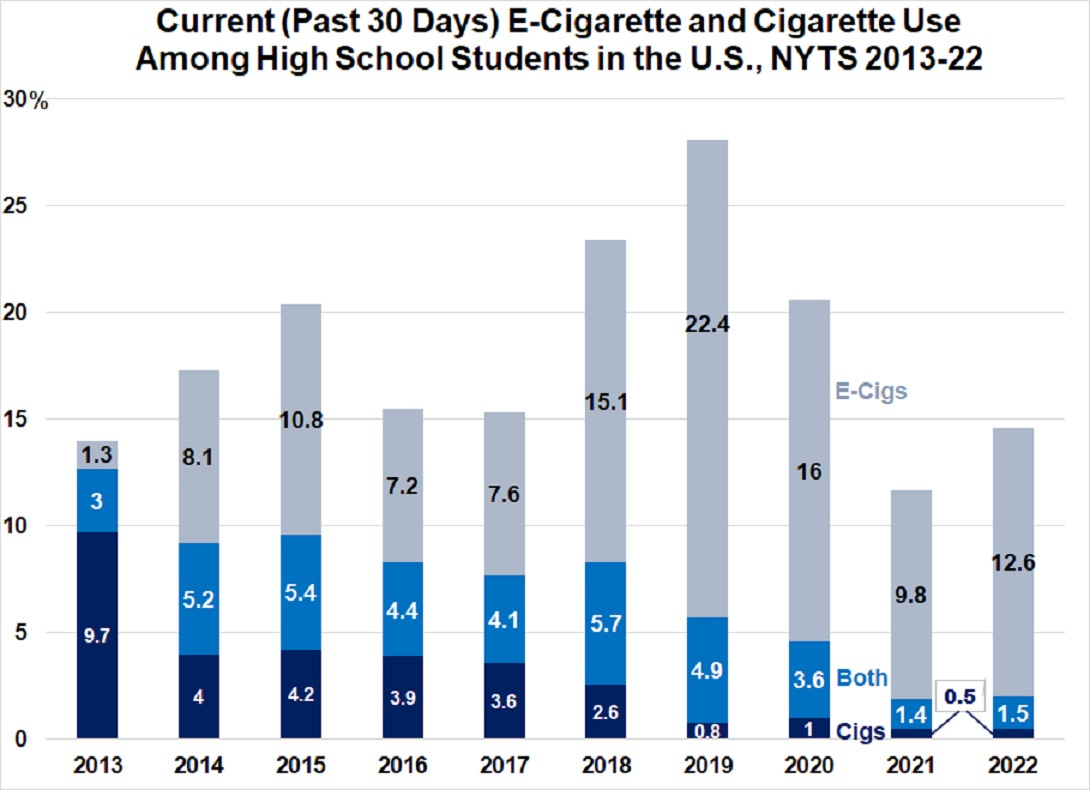
Vaping is not a gateway to smoking: youth use cigarettes in historically low numbers. Only 2 percent of high school students smoked at least once per month in 2022, with 0.5 percent of high school students using cigarettes and 1.5 percent smoking and vaping in addition.
As for teen vaping in 2022, 14.1 percent of high school students used an e-cigarette at least once in the last month (12.6 percent use only e-cigarettes, 1.5 use both cigarettes and e-cigarettes) and 4.2 percent of high school students use daily. (NB: CDC data show that 30.1 percent of high school vapers (14.1 of all high schoolers) use daily. 30.1 percent of 14.1 percent = 4.2)
We must maintain perspective: The vast majority of teens, about 86 percent of high schoolers, don’t use e-cigarettes at all. If anything, vaping has displaced smoking in high school youth (even been a gateway out of smoking for some) . See graph below for trends since 2013.
Another concern cited were claims of nicotine-induced harm to the teen brain, based in part on studies of the brains of adolescent mice. Their brains do show neuronal alterations, but what those changes mean for human teen brains is far from clear.
Other evidence relies on examinations of cognitive function in teen smokers. These are cross-sectional studies that are confounded by the established connection between youth smoking and pre-existing problems that are correlated with deficits in cognitive performance, such as conduct disorder, mental illness, and high school drop-out rates. What's more, evidence suggests little correlation between IQ and smoking status.
As one science journalist aptly put it, “The American public essentially conducted a massive experiment on this very subject in the mid-1960s, when 52 percent of men and 34 percent of women smoked. In the decades following, there was no evidence that similar proportions of the total population had become brain damaged.”
Conversely, nicotine has virtues. Here is an impressive bibliography of articles on the benefits of nicotine, part of this website on safer nicotine, which is compiled by volunteers.
So what do we know? Youth should not vape. Adults should not smoke. And, in the words of a comprehensive “comment” out in Nature this month, “Because of the uncertainty about the risk of using e-cigarettes long-term, former smokers should plan to quit e-cigarettes eventually but only when they are confident that they will not go back to smoking combustible cigarettes.”
These imperatives need to be taken into account with appropriate trade-offs made. The U.K. knows this best. The National Health Service is considering provision of free vaping starter kits to “deprived communities” and is now subsidizing vaping for its own staff as a pilot program. Here is what U.K. anti-smoking groups offer youth and here is an excellent 12 minute explainer from the Economist, featuring Robert West, Professor of Health Psychology at University College London and former Editor-in-Chief of the journal Addiction.
One could see campaigns in the U.S against vaping as nothing short of a gift to cigarette makers. Every alarmist news article and public service announcement, every “vaping-is-dangerous” journal article, every new tax on vaping, and every heavy handed regulation redounds to the benefit of cigarette makers. Smokers scared of switching, doctors misinformed by otherwise trusted health advocacy groups, and vaping manufacturers that cannot afford the vast expense of required pre-market tobacco applications to the FDA means continued smoking by millions.
The e-cigarette story is a dire chapter in the sociology of public health science. In the future, however, it could prove to be an instructive one as well. If there are any grounds for optimism in the long run, they come from abroad.
Public health authorities in England, where harm reduction as a general policy has long been embraced, endorse and promote vaping as a harm reduction strategy for smokers. As nations that embrace (or at least do not actively discourage) vaping save smokers’ lives -- and as illicit vaping markets take root here -- American policymakers will be forced to notice and adjust their risk-benefit calculus and their policies accordingly. They will need to acknowledge, too, that many of the same activists who fought heroically against the deceptions of Big Tobacco, were the same ones who thwarted a nascent health revolution, slanting science to fulfill their own prohibition mission.
 | A guest post by
|
This is just another nail in a very ugly coffin for anything in the US described as "public health". There has been literally nothing that public health, writ large, has done that is really constructive over the past five years. Please do not whine to me about how everyone works so hard and wants the best things to happen. Covid is an even better example of the disaster that "public health" is, but the list is long, including the vaping issue.
If we wish to make America healthier, the right place to start would be completely dismantling the current "public health" structures and (if people insist) starting over. Clean water, etc. are in a different category and have been addressed well for 100 years. But vaping, vaxxing, diets are part of medicine -- not community cleanliness. Since medicine is an n-of-1 profession, it is unclear how much benefit population measures homogenized by governments led by those with other agendas will ever do. And the tendency of "public health" to squelch all dissenting opinions is reprehensible at best and lethal at worst -- as we are increasingly finding out.
Personally, I believe that the worst part of the "public health" debacle is that it has taken down the medical profession with it. After decades of gaining people's trust, patients now disbelieve much of what we physicians say...and I cannot blame them. Some of that belongs to each practitioner who (AB2098 before the law) just recited the government pabulum -- although some of us did not. But a lion's share of the loss of trust belongs to the NIH/CDC/FDA axis that promotes things that most normal people can detect are just wrong. (Note the number of boosters given, or the continuing strength of vaping.)
It will be decades if forever before medical practice/health care regains the credibility many of us have worked hard to earn to provide the best care we know how for our patients. If "public health" remains as it is, it will NEVER happen. People are now in the "fool me twice" position. They know better.
With all due respect, as the mother of 3 peri-adults, the incidence of e-cigarette use is dramatically higher than this data suggests. All 3 of my children (ages 18,20, and 22) use it to varying degrees (much to my despair, and my fear mongering with my 2 boys that nicotine use is a leading cause of ED later in life) and they will tell you that “99% of HS age kids use it”... no matter if their social, academic, or athletic status. My kids ran/run with a variety of kids, not just one group. They were all high level athletes (1 will play a division 1 sport in college). It is pervasive and they lie about using it.