
Workplace culture: Reader Input Needed
A cardiologists switches universities and no one shows up, what is going on?

Recently, a colleague of mine switched institutions. He works as a faculty in cardiology, and attends on service with fellows. Over the course of the year, he gives scattered lectures on the interpretation of clinical trials. I think it is fair to say he has similarities to John Mandrola— a consummate cardiologist and clear evidence based thinker.
When my colleague switched institutions he noticed some differences in culture. At his old institution, there were in-person lectures, every Friday, for the fellows, and faculty were encouraged to join (he did)— in the new one, these were on zoom, and faculty were not invited. At the old institution, faculty would come to the office and sit and work on their computers, when not in clinic or on service— now, they worked remotely. At the old institution, there were quarterly dinners or barbecues or potlucks at one faculty member’s house, where the entire division was invited, at the new institution these did not occur.
A few other differences:
At fellows graduation dinner: The old institution had near 100% attendance from other fellows (of different years), and near 100% attendance of faculty in the division. At the new institution this was ~20% of fellows not graduating and 20% of faculty.
At fellows graduation: Each fellow typically had a faculty member they worked with most closely, and these faculty gave speeches for the graduate. At the old place, 100% of speeches were in person. At the new place 50% of faculty emailed a zoom recorded video and were not present.
At the old institution, there were division wide grand rounds with invited speakers, and faculty would take turns going out to dinner the night before with the speaker— at the new place there was no such grand rounds series and naturally no dinners.
At the old place, there was a single fellows room with couch and refrigerator, and faculty would occasionally stop by to chat. At the new place, there was no such room, but moreover, fellows would not be at work unless in clinic or in lab— otherwise it was work from home.
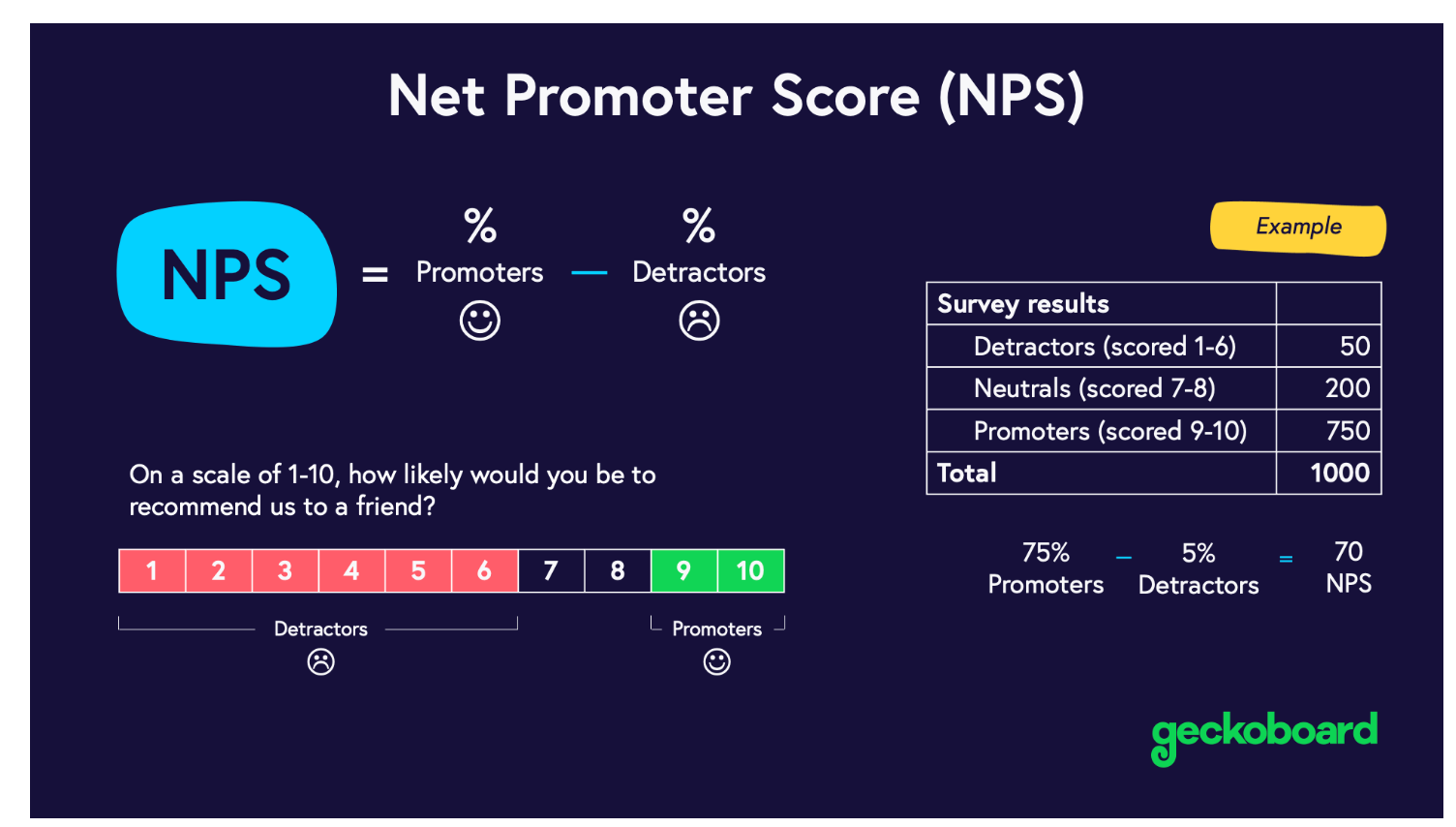
At the new institution, the net promoter score was -100
My colleague doesn’t know what accounts for this. One possibility is pay— the new institution pays slightly less than the older one, but it is a modest difference. Another possibility is metrics— the new institution more slavishly adheres to boosting RVUs. Another is leadership, the old institution had a well liked chief, and the new one has someone who exhibits traits of narcissism.
I am truly not sure. While it is clear to me there is a pattern of differences, and it appears cultural, I am not sure if it can be boiled down to a single factor. Moreover, I am not sure what the solution is. Neither is my colleague.
So I turn to the wise readers of Sensible Medicine to guide him. What do you think? What accounts for workplace culture like this? What are the causes, but more importantly, what are the solutions? And, if you enjoy what we are doing with Sensible Medicine consider becoming a paid subscriber.
As you say, many causes. But there is one overriding theme: in person matters.
There are many people who have become (IMO) invested in the concept of remote being an acceptable substitute for in person i have seen this in medicine, where some colleagues rounded almost exclusively from home, and at a startup I was part of. It had its soul sucked out by the switch from a robust in-person culture to mostly-remote.
We can debate the merits and necessity of this during the first year of the pandemic, but at best it should have been a necessary evil until vaccination.
Instead it has persisted, and I think it is worth exploring why:
1. Comfort. I am not immune, to say the least. Human interactions cause a bit of anxiety for many of us. It is so _comforting_ to have the mask (and the ear buds) (and the shades) and be an island. Zoom has very little of true social interaction, and if things get tense (or any other thing draws our eye) then “camera off” fixes it.
The issue: all of the best things in life happen outside of our comfort zone. Friendships. Confidences. Even the misunderstanding or strife that leads to bonding later. These are greatly reduced in remote.
2. NPC syndrome: I saw this in earnest at that startup. There was a huge blowup against the CEO over our…insufficiently-robust…response to the George Floyd murder. People behaved shabbily, and in a way they would not have done in person. People on a screen just don’t seem real. So why show them IRL respect?
3. Let’s be honest: it’s not just the commute that makes WFH easier. We are less engaged (ok, not all, just the majority of us. Some folks are suited to remote and I salute them.) (Most people who think this describes them are wrong). We are quick to take a break or task switch. We do less deep work, and, I believe, less work overall.
People like remote work because it is comfortable, nobody seems real, and who doesn’t like the same pay for less work. We’d _like_it to be just as good, so we find ways to justify it. But we are fooling ourselves.
So: I think this new institution has a bad culture that starts w poor leadership. This has been abetted by the normalization of remote work. Making people show up won’t, by itself, fix the culture, but if people don’t show up, _nothing_ will fix the culture.
We are social creatures. In. Person. Matters.
Most of the comments echo my thoughts. The culture of today hinges on google searches-less actual human to human interaction--more digital intervention..more ghosting while even on the job. I am a retired RN who was military and in the past trained nurses, residents, and fellows. The culture has definitely changed to here and now to get by. Lively medical rounds are gone, creative out of the norm medical thinking is gone, responsibility as a medical team is gone. Remote from home and AI-so we don't have to think hard-robotic surgery have given the opportunity to not hone expert technique in training physicians, not have lively discussions about treatment, and not know the people we work with. The young medical profession including physicians and nurses would rather google for an answer by themselves than ask a colleague for help. I recently recommended to a physician teaching trauma medicine to take all the "techy tools-stethoscopes, pulse oximeters. telemetry, FAST ultrasound and make his students actually look at the patient to assess, ask questions of the patient, actually read past hx notes--not just the summaries--figure out how to treat the patient without googling. As an old RN who deployed, I am terrified of how our medical teams are being trained. No wonder we did not get it right in the US during COVID.