
“Doc, I got a MyChart alert that I am due for an RSV vaccine, can I get it today?”
How should a doctor respond? An essay and a poll.

You have received an alert through your patient portal that you are due to get the RSV vaccine. The recommendation is based on the CDC’s guidance that all adults aged 75 and older receive a single dose of the vaccine.1 You see your doctor, let her know that you got the alert, and you want to do what is right. You ask her for the shot. How do you want the doctor to respond, with certainty or with nuance?
I’m embarrassed to admit that this question came to me not in clinic, where my patients bring up their MyChart alerts with me every day, but after I read the latest RSV vaccine article and discussed it with John Mandrola and Andrew Foy on This Fortnight in Medicine XXIV.
The NEJM article described a beautifully conducted RCT in which 131,276 people were randomized to receive the RSV vaccine or remain unvaccinated (no diluent or saline comparator here). The primary endpoint was hospitalization for RSV-related respiratory tract disease. The secondary endpoint was hospitalization for RSV-related lower respiratory tract disease and hospitalization for respiratory tract disease from any cause.
The randomized patients had a mean age of about 69, and about 80% had the flu vaccine the year before and the year of the study. 42% of the patients were being treated for a chronic disease.
The RSV vaccine was, as we like to say, safe and effective. Over six months of follow-up, the vaccine effectiveness for the primary endpoint was 83.3% (42.9-96.9). For the secondary endpoint, hospitalization for respiratory tract disease from any cause, the effectiveness was 15.2% (0.5-27.9). The incidence of serious adverse events was similar in the two groups.
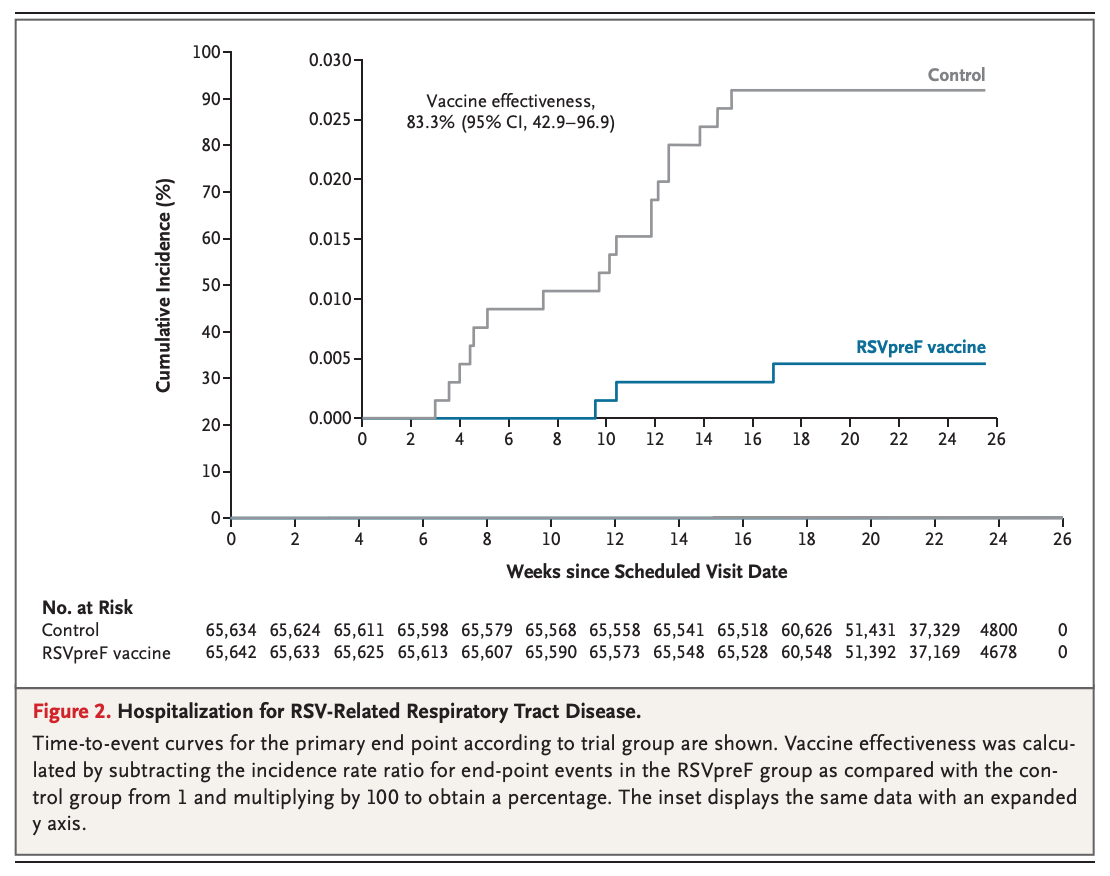
When we look at absolute differences, rather than the relative differences described by vaccine efficacy, the numbers tell a somewhat different story. Hospitalization for RSV-related respiratory tract disease occurred in 3 of 65,642 participants in the vaccine group compared with 18 of 65,634 participants in the control group. That is a number needed to vaccinate (NNV) over six months of 4376. (For the secondary endpoint, the NNV is 1286).
The TLDR of all this is that the RSV vaccine is safe and effective, but the real question is whether RSV is a big enough problem to vaccinate every human over 70. As always, there are two arguments that can be made.
If you are pro-RSV vaccine, you’d argue that while a 1/1300-4400 chance of avoiding a hospitalization doesn’t seem impressive, it is impressive from a population standpoint. An intervention that decreases hospitalization by 1/1300 is pretty good. You’d also point out that these NNVs probably understate the benefit. If these numbers repeat themselves every 6 months, after 10 years, you’re at a NNV of 65. Preventing a hospitalization in the next 10 years in 1 of every 65 people you vaccinate is incredible. While we’re madly extrapolating data, you might also suggest there is a 3rd party effect.
If you’re anti-RSV vaccine, you’d argue that a doctor’s role is to care for individuals, not populations, and that the data at hand should guide us, not extrapolations that may or may not be reasonable. In this case, it should be the patient’s choice whether he wants a shot that will decrease his risk from 1 in 3612 to 1 in 21,667.
Let’s get back to the MyChart alert. The RSV recommendation stems from our current approach to healthcare: if a safe treatment is beneficial, even if the benefit is small, we recommend it. This rationale is behind the new lipid management recommendations for low-risk people and explains the heaps of money the US spends on health care for outcomes worse than those of our peers. I think that taking this approach to healthcare is probably right for some people, wrong for others, and wrong for society. But that is just one opinion.
When a patient comes in asking for a test or treatment because it has been recommended by the electronic health record (a stand-in for someone making clinical recommendations), the doctor could respond in two ways.
She could say, “Yes.” This respects the national guideline. It also assumes that the patient has considered the recommendation and decided that it is right for him. It is also patient-centered. You asked me for something, it is not an unreasonable request, and I am going to satisfy it.
Or the doctor could say, “You can certainly get it today, but would you like to hear more about the magnitude of the shot’s benefits?” This response leans into patient education and shared decision-making. It is also time-consuming and undercuts the authority of national bodies. It also might be confusing to a patient who assumes the EMR alert reflects his doctor’s decision-making. It also might come off as antivax. “You really want a vaccination? Maybe you should reconsider.”
So, loyal reader, how would you want your doctor to respond if you said, “Doc, I got a MyChart alert that I am due for an RSV shot. Can I get it today?”
A. Yes.
B. “You can certainly get it today, but would you like to hear more about the shot’s benefits?”
Some personal follow-up
