
Friday Reflection 44: Diagnostic Enigma

PJ is a 53-year-old woman referred for a consultative visit. For the last 12-18 months she has been suffering from fatigue, headache, joint pain, and rashes. She has been seeing a primary care internist and has had consultations with a neurologist, a dermatologist, and a rheumatologist. She presents with a folder of records and codes for outside EMRs.
Ask general internists what they love about their field, and they are likely to talk about long-term relationships with patients and the pleasure of solving clinical puzzles. I feel most like I am “among my people” discussing diagnostic dilemmas with my team post call.
Internists are not alone in their love of the clinical puzzle. The Medical Detectives by Berton Roueche is a beloved classic. Lisa Sanders has made a career — beyond her medical practice — of engagingly describing struggles to solve difficult cases. Many of my non-medical friends have asked me to recount interesting cases.1 House, a show I loved because the stars were doctors (actors playing doctors), sitting around a whiteboard, usually featured some great clinical conundrums.
What makes a diagnostic dilemma? The overwhelming majority of presentations are routine, easily solvable. A patient has a common disease presenting in an expected manner. If there is uncertainty, it is because there might be a few common diseases, all of which present in similar ways. A healthy, middle-aged person with subacute, intermittent, epigastric pain might have peptic ulcer disease, non-ulcer dyspepsia, or cholelithiasis.
Diagnostic dilemmas are those that occupy the other three squares of a 2X2 table.2
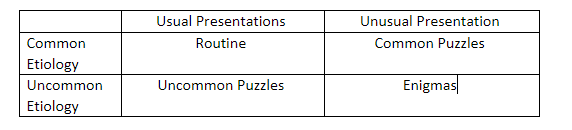
Common puzzles test diagnostic reasoning. They demand that you know alternative presentations of common diseases and recognize that, given their incidence, they will not be unusual. This is the migraine presenting as episodic nausea, or pyelonephritis presenting with right upper quadrant pain.
Uncommon puzzles test knowledge of differential diagnoses. It is knowing that after you have excluded the common causes of thyrotoxicosis, it might be worth inquiring from where the patient is getting his ground beef.
Enigmas are the diagnoses you remember. They are diseases you rarely diagnose, presenting in one of their less common ways. It is when you diagnose amyloidosis as the cause of a peripheral neuropathy, or find that the cause of a patient’s anxiety is hyponatremia, caused by SIADH, caused by a radiologically undetectable lung cancer.
An example of an enigma
RS was a 60-year-old man who came for an initial visit with fatigue. Because fatigue is such a nonspecific concern, the visit was spent trying to discover another symptom that could narrow the differential diagnosis. There were none.
The fatigue, however, was unusual. For six weeks, there were episodes, three times a week to twice a day, of overwhelming fatigue. During these episodes, RS had to put his head down on his desk. He did not sleep during these periods but felt “spacey” and wiped out. There were no palpitations, dyspnea, or other associated symptoms. There were no triggers. The episodes lasted from five to fifteen minutes.
After about ten minutes of interviewing, one question opened the door to a diagnosis.
“Do you notice any unusual smells or noises before the fatigue?”
“Actually yes. For the last couple of weeks, I’ve been noticing a foul odor right before the episodes. By the time I feel better, I no longer smell it, so I have not investigated the source.”
This suggested partial, complex seizures with a post-ictal period. His exam was unremarkable, but an MRI demonstrated a small glioblastoma multiforme. Certainly not a diagnosis to celebrate, but a solid one nonetheless.
I am presented with diagnostic dilemmas either by an established patient with a fresh concern or by a new patient with a problem that has not been solved by other doctors.
These unsolved chronic problems are never easy. In American medicine, easy access to advanced laboratory assays and innovative imaging means that even a middling doctor usually stumbles into a diagnosis.
PJ had already been seen by multiple doctors, one of whom I knew and might go to if I were experiencing perplexing symptoms. Most of the diagnoses that I would have considered had already been evaluated.
Over the years, I’ve developed my own approach to patients like PJ. Although it is said that good writing shows rather than tells, I’m just going to tell you my approach.
At least initially, don’t get obsessed with chasing zebras. Clarify whether the problem is that an accurate diagnosis has not been made, or that a diagnosis has been made but has not been accepted. I’ve seen many patients who shop around for a diagnosis because they are unwilling to accept the true diagnosis that has been made. Always ask, and ask again, about alcohol and drug use. The adverse effects of illicit substances, in terms of both symptoms and objective medical findings, are legion. So many people are loath to admit habits and addictions, even to a doctor, even when it would be in their best interest to do so.
Always ask the patient what he thinks is causing his symptoms. Even with a patient who has been seeing another doctor for a while or has seen many doctors, no one has put as much thought into their symptoms as the patient himself. These days, the attention is likely to be more than idle pondering; it's likely to be actual research. Accept that the patient knows more about his symptoms and may very well know more about his disease than you do.
Next, take your time with these cases and put in the work. On every clinic day, there are visits that take more time than allotted and others that take less. Let enigmatic visits run long. Take your time collecting the medical history, doing the physical exam, and reviewing the reams of outside records that are sure to accompany the patient. Take a good family history, looking for histories of psychiatric disease, early-onset dementia, and rheumatologic diseases — things other doctors might have shied away from and that patients might not know well.
My habit is not to order tests at the first visit. I like to write a detailed note to help me think about the case before testing.
If I get to this point without a solution, it is time to consider interesting diagnoses. Most of the time, the answer is one of the great mimics: generalized anxiety disorder, depression, celiac disease, sarcoidosis, SLE, hypermobility spectrum disorders, POTS, ovarian cancer, diabetic amyotrophy, TB…
Lastly, in these situations, Hickam’s dictum is often a better guide than Occam’s razor. This was the case with PJ. Multiple issues were causing her symptoms. Her diagnosis was made almost entirely from data available on her history and physical exam. Her symptoms were explained by a disease — seronegative rheumatoid arthritis — together with the adverse effects of medications that had been added over months to control her symptoms, and an adjustment disorder, a reaction to her year of lost function.
Usually, the doctor alone appreciates a “great diagnosis.” The patient has come to the doctor with a problem to be solved. When it is solved, the patient feels like she “got what she paid for.” It is only the doctor who thinks: what an interesting presentation: I’m pretty impressed with myself for making the diagnosis quickly and parsimoniously; will one of my colleagues be interested in listening to me congratulate myself?
PJ is the exception. She asked me to write up her case.
This never works out well. I am uncomfortable talking about my patients, and the narrative of the cases I’d share would be short compared to the time I would need to explain why the case is interesting.
I feel rather pathetic that it has been since December 2023 that I’ve been able to sneak a 2X2 table into a Friday reflection!
I'm a primary care internist, too. I'm impressed and enjoyed the article which was much more than listening to you congratulate yourself!
I could not agree more about asking the patient what they think is causing the symptoms. Another reason to ask that is that sometimes the symptoms become quite bearable if you tell them it's not elbow cancer or whatever their worst fear was.
The thing I have noticed (and have gotten better about detecting now nearer the end of my career than the beginning) is how frequently the "mind body syndrome" plays a role in a wide variety of symptoms. I find it fascinating, that after the initial evaluation (and some follow up) is done, that it becomes quite easy to see where the patient's thought process is leading to their symptoms. When you've spent a lifetime listening to humans tell you about bodily things, you have a broad array of the typical and you can spot the less helpful thought processes. The issue I have with this problem: it takes TIME to determine and time to gently help the patient gain insight and tools to manage. For the amount that I see in my practice, it makes me realize that a significant portion of health care dollars are spent running down issues related to MBS or other similar problems (medical PTSD; adjustment disorder; etc). Current health care is doing its part to drive this problem as the 15 minute visit along with the plethora of tests we have at our disposal, just masks this problem and fuels its fire. The other issue is the underlying movement towards AI and "chatbots" getting highly involved in medical care will not help this problem either. Human beings are not soothed or reassured by algorithms - human connection and really listening are the cure.