
Is Universal Testing for Lp(a) Warranted?
I Have Questions

There has been lots of commentary on the 2026 Lipid guidelines. John Mandrola, Andrew J Foy, and Venk Murthy even did an “emergency podcast” on the topic which broke all download records for us. One thing that I think has been covered less is the recommendation for Lp(a) testing. Here, Dr. Marine offers a very sensible take on the issue.
Is Universal Testing for Lp(a) Warranted? I Have Questions.
I recently received a distressed email from an internist colleague and friend who was upset by the results of a blood test (lightly edited to anonymize):
“I slept poorly last night. [My PCP] wrote me a note saying that I had to tell all my first-degree relatives to get checked for Lp(a) and that I should have coronary calcium scoring. It weighs heavily on me that I could have passed this on to my kids. Because there is nothing to do about it, I feel like it’s my death sentence.”
I wrote back to better understand the cause of such intense feelings. Turns out that my colleague had expressed concern to her doctor about her family history. Her father had an aortic valve replacement for calcific aortic stenosis in his early 70s and recently died from prosthetic valve degeneration. She also had 2 other relatives who had clinical atherosclerosis and ischemic strokes in their later years. She wanted to better understand her cardiovascular risk and how she could mitigate it. So, her doctor ordered an Lp(a) test. It came back “High” (scary highlight original):
I had been hearing about Lp(a) as a risk factor for atherosclerotic cardiovascular disease (ASCVD) and calcific aortic stenosis (AS) for several years. This association had long been known and more recently clarified by several large database studies showing a correlation with cardiovascular risk. The mechanism by which Lp(a) causes increased risk remains incompletely understood. The talks usually ended with excited anticipation of trials of new pharmaceutical products which lower Lp(a) - none of which have yet been completed or reported.
So why is Lp(a) measurement being promoted now when there is no specific treatment for it? I turned to the recently published 2026 ACC-AHA Dyslipidemia Guidelines for some answers:
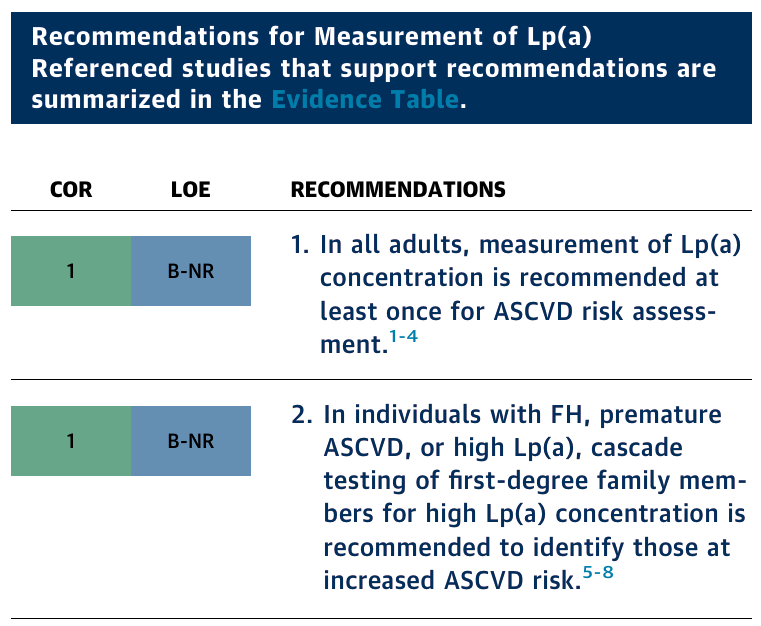
A cardiologist colleague also provided this nice infographic:
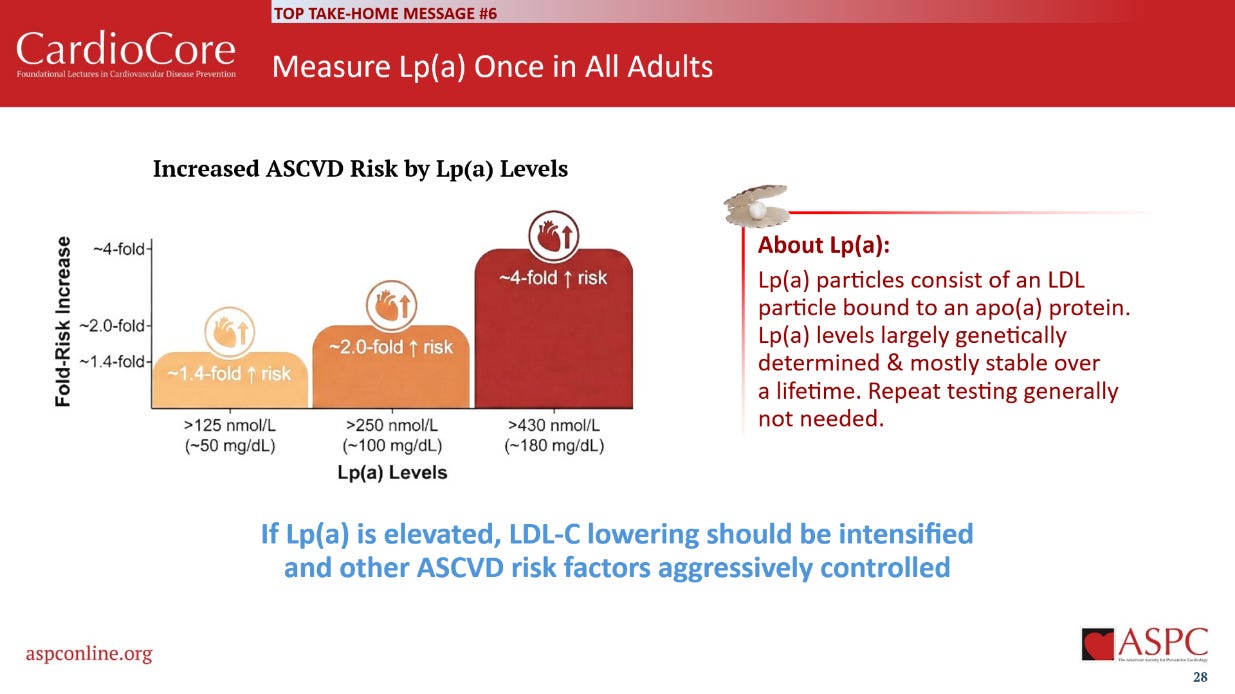
But this information just led to more questions and concerns:
1. What is the benefit of a test without a clear plan of action based on the test result? Such testing may just cause non-productive anxiety and distress. Labeling patients with a new disease (? Lp(a)-itis) has psychological consequences, especially if there is no specific treatment for it. The guidelines suggest using Lp(a) as a “risk enhancer” to select patients for more intensive lipid-lowering with current drugs but provide no evidence that this application of the test improves patients’ health or outcomes net of the cost and harms. Interestingly, the most commonly recommended and prescribed lipid-lowering drugs, statins, have little effect on Lp(a) levels.
2. The universal testing recommendation is made outside of any Bayesian framework. A “40% increased risk” can sound scary to someone worried about their cardiovascular health. But if that person’s baseline 10-year absolute clinical risk of an ASCVD event is only 2% (the case with my colleague), then a “40% increased risk” translates to an absolute risk increase of less than 0.1% per year – clinically meaningless. Pre-test probability matters. Absolute risk matters. This is clinical reasoning 101. For most patients with low baseline risk, reinforcing Life’s Essential Eight lifestyle prevention may be more healthful and empowering than pointless lab testing.
3. The universal recommendation for measuring Lp(a) creates an impression (a false impression, I hope) that the medical profession has been enlisted to prepare a market for new pharmaceutical products which have yet to show any net clinical benefits for actual patients. If the trials of these products fail, what happens to the class I testing recommendation? Will it need to be revised? This would raise questions about why it was made in the first place and undermine public confidence in other guideline recommendations.
4. There have been many markers of risk for all kinds of diseases, conditions, and outcomes that have emerged from database research and mechanistic studies. Only a small percentage make their way into clinical practice. In my field of EP, they have included microvolt T-wave alternans, baroreflex sensitivity, and heart rate variability. Most fail when put to the ultimate challenge: Does the test improve healthspan or lifespan net of costs and adverse effects? There are many tests which predict sudden death risk, but few that have met the latter challenge of clinical utility.
In our medical training, we are programmed to rely upon testing. Medical students and interns learn the ritual of “morning labs” on every hospitalized patient. Repeated checks of potassium and magnesium levels on every cardiac patient getting diuretics (remember those nursing calls at 2AM for K of 3.4?). Lots of X-rays, CTs, and MRIs. When in doubt (and medical trainees have lots of doubts), do more tests.
Academic specialists should also be sensitive to the burdens placed upon primary care clinicians. When academic specialists make a new universal screening recommendation, someone else (usually) has to fulfill it. This is the classic unfunded mandate. Primary care specialists are already inundated with hundreds of screening and other preventive measures they are encouraged to perform and interpret for large numbers of patients, in addition to managing their acute and chronic medical problems. Patients are also bringing them results from genetic tests, wearable device data, and whole-body scans the primary care doctor never asked for. Little wonder that there is so much burnout in the field. Academic specialists should therefore ensure that new broad screening recommendations imposed upon primary care clinicians and the public are fully warranted and evidence-based.
So, what am I going to do with Lp(a)? Based on my experience and review of the data so far, I will not be rushing to test all my patients for Lp(a). I will look forward to critically examining the clinical trial results of Lp(a) lowering drugs. Does this make me a bad doctor, or a sensible one? I will let the reader decide. What do you think?
Dr. Joseph Marine is an arrhythmia cardiologist who practices in Baltimore, Maryland.
 | A guest post by
|
This is a fantastic overview. One of the lowlights of a typical clinic day for me is a patient bringing in an elevated Lp(a) someone else ordered. Whatever happened to the maximum "Don't order a test unless you know what you're going to do with it"?
Thanks for the well reasoned commentary.
The suspicion that universal testing ( including first degree relatives!) is a ploy for future pharmaceutical sales is well founded. Seems Lp(a) testing should be confined to research settings until an effective treatment exists and it shows absolute clinical benefit that outweighs the risk and cost. A marginal improvement at enormous expense is worse than no treatment at all.