
Observational Studies in Pregnancy, Autism, and Politics: What Could Possibly Go Wrong?

When people send me a message to tell me that they’d like to read about something on Sensible Medicine, I generally respond, “I would too. Could you write it?” That often ends the conversation. After about a dozen messages, I had to admit this topic was in my wheelhouse. I’m writing about it for the medicine and the critical appraisal, not for the reasons that seemed to underlie a lot of the requests.
Medicine, Medicines, and Pregnancy
The role of medicine in pregnancy is quite a topic. How a male-dominated profession cared for pregnant women (who mostly do fine taking care of themselves) in the 19th and 20th centuries has filled many a thesis. Fortunately, the human body has evolved to protect the next generation; fetuses are seldom affected by what goes on around them.
Though not completely.
We have learned about the effects of alcohol, thalidomide, isotretinoin, DES, lithium, and many other therapeutics. Our knowledge has made us extremely cautious about what we recommend to pregnant women. Throughout my career, the general recommendation has been to administer as few medications as possible, especially during the first trimester. Pregnant women presenting to an urgent care are sure to send doctors to Medscape to check the “safety in pregnancy” tab for drugs they would usually prescribe without a second thought.
This has not always been the best thing for the pregnant woman and her unborn child. We have undertreated some women out of fear, to their detriment and possibly to the detriment of their children. Our reluctance to use safe medications to treat pregnant women with depression and seizure disorders comes to mind.1
Studying the adverse effects of medicines in pregnancy is incredibly difficult. Highly toxic effects of medications can usually be delineated through case series. The ill effect of DES, whose damage manifests when the former fetus reaches adolescence, was determined in a brilliant case-control trial.
Randomized controlled trials cannot be done to investigate harm, especially in pregnant women. Even if we abandoned all morality, the numbers necessary to find the small number of babies affected, sometimes later in life, would be prohibitive.
Mostly, we rely on observational studies. Case-control studies match affected and unaffected children and look backward at exposures. Cohort studies enrol exposed and unexposed populations and then follow them, waiting for diagnoses to be made. Both of these designs are prone to measurement bias, primarily concerning the accurate determination of exposure. Even if they are done well, observational studies prove correlation, not causation. Women who take medications, any medication, during pregnancy are different from those who do not. If the woman are different in important ways, their offspring are likely to be different. This is confounding.
Autism
I am pretty convinced that there has been no increase in autism in the last 50 years. I should restate that: there has not been a major increase in autism, and if there has been an increase, it has been too small for us to detect.
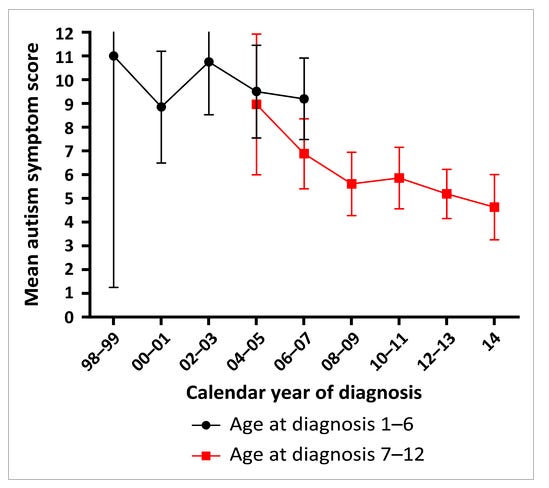
What has happened is that there has been a rise in awareness of the disease and an enormous broadening of the diagnostic criteria. There are lots of great papers on the topic. My brief, and hopefully acceptable, take is that from 1994-2013, Asperger’s Syndrome was included in the DSM. Some children who received this diagnosis were truly disabled, others (and I say this lovingly and with no ill intent) were just quirky. In 2013, Asperger’s disappeared, rolled into autism. This evolution swelled the roles of those diagnosed with autism. There has been some outstanding research demonstrating that as the number of people with autism increased, the number of symptoms displayed by people with autism decreased. Here is a figure showing this from an article by Olof Arvidsson, Christopher Gillberg, Paul Lichtenstein, and Sebastian Lundström:
Acetaminophen and Autism
Autism, in its traditional presentation, is a terrible condition. It is frightening to parents. Even if the “epidemic” does not exist, autism is an important medical issue. The research, which I do not follow closely, suggests that the autism’s etiology is complex.
Political leaders make promises. King Henry IV promised “a chicken in his pot every Sunday”. John F. Kennedy promised that we would reach the moon in a decade.2 For some reason, last April, RFK Jr. promised us that we would understand the cause of autism by September. I expect that promise was behind this week’s announcement of the link between fetal exposure to acetaminophen and autism.
The data that underlie this “discovery” are summarized in a review article published on August 14, 2025 in Environmental Health. This is a review article, not a meta-analysis. Meta-analyses use quantitative methods to summarize results. In this article, there is no attempt to determine summary risks or assess the heterogeneity of the data. Even a perfect meta-analysis that revealed a relationship between acetaminophen and autism would leave us only with an association, not proof of causation. Only evidence of causation suggests that an action will be effective.
Some points on the data.
The article investigates the relationship between acetaminophen exposure and both ADHD and autism. These are entirely different diseases. The fact that the paper finds an association between acetaminophen exposure and both “neurodevelopemental disorders” suggests confounding rather than causation.
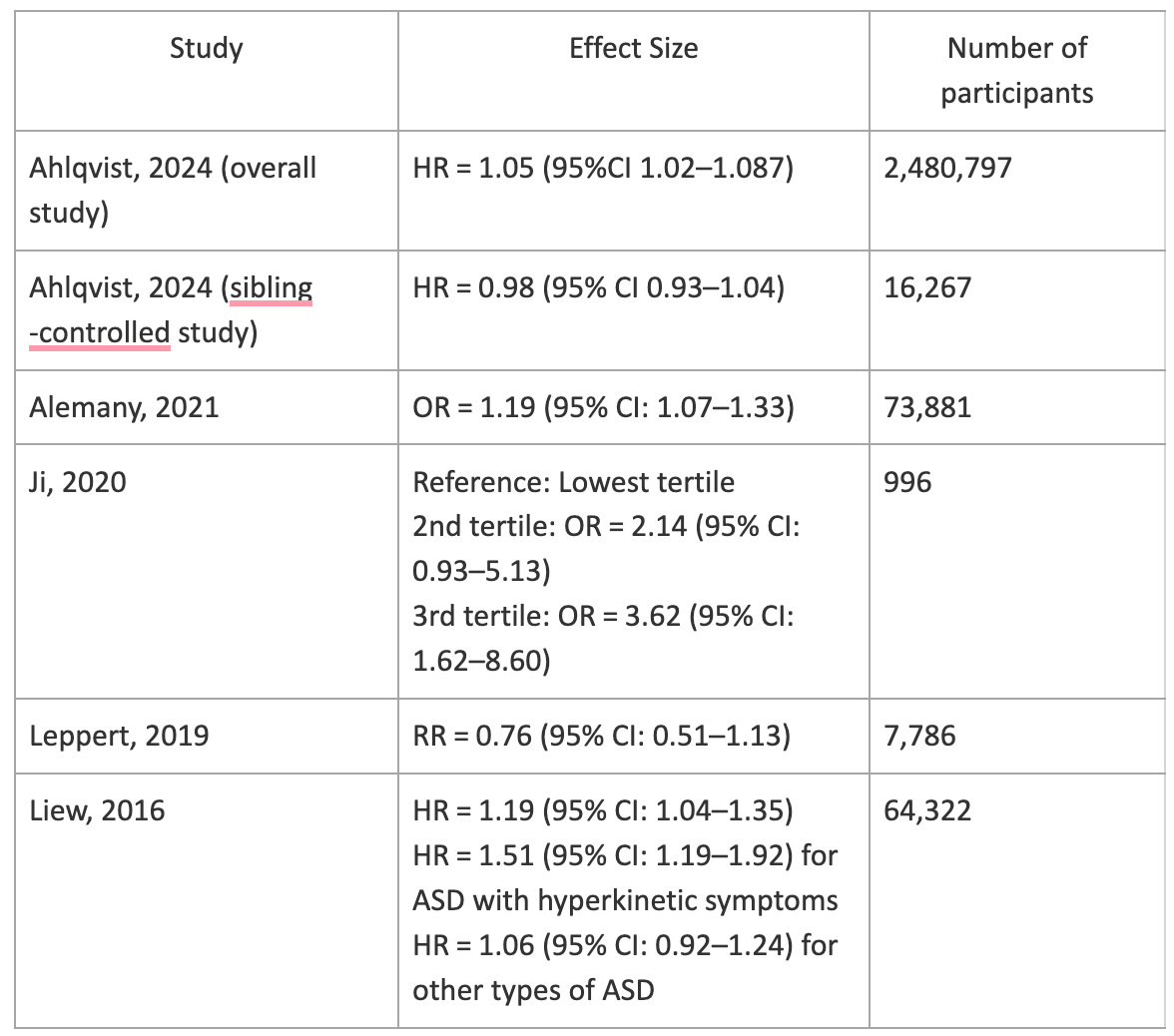
The effect sizes (really just relationships) are small and often insignificant. Given the confounding expected in even well-done observational studies, it requires large associations to make them important. This table summarizes the findings from the cohort studies included in the review.

The conclusion of the review makes me very concerned about the impartiality of the authors and the intention of the editors:
“Our analyses using the Navigation Guide thus support evidence consistent with an association between acetaminophen exposure during pregnancy and increased incidence of NDDs. Appropriate and immediate steps should be taken to advise pregnant women to limit acetaminophen consumption to protect their offspring’s neurodevelopment.”
It will be fascinating to see what emerges about this process in the coming weeks and months.3
Conclusion
Last week, most physicians, including myself, told women to be cautious about medications during pregnancy. We would have given them a list of medications that they could use if needed during pregnancy. This list would have included acetaminophen.
I guess, in his own way, this is the advice that President Trump gave in the linked news conference.
That said, we are no closer to knowing the cause of autism. We are no closer to understanding how to decrease the incidence of this disease. We are further from people trusting science, or at least understanding that not all scientific findings are equally trustworthy. We have left pregnant woman even more uncertain about how best to care for themselves and their baby during pregnancy.
This is a reversal study we never got around to writing. The classic medical reversal occurs when a practice, adopted based on flawed data, is found to be ineffective or dangerous. Another type of reversal happens when a practice is withheld due to suspicion that it is unsafe. When robust data reveals that it is safe, we realize that we injured patients by withholding an effective therapy.
“We choose to go to the moon in this decade and do the other things, not because they are easy, but because they are hard, because that goal will serve to organize and measure the best of our energies and skills, because that challenge is one that we are willing to accept, one we are unwilling to postpone, and one which we intend to win, and the others, too.”
If journalists are looking for a scoop, spend some time with these authors and editors. If you find something juicy, I’d at least like an acknowledgment.
Photo Credit: Volodymyr Hryshchenko
In the 1960s when I started school and grew up, autism was very rare. Now, we know numerous kids who are not just a little on the spectrum — they are barely verbal. Their parents are now saddled with a terribly disabled child, for life.
There is zero question to anyone like me, growing up with their eyes open, when we did, that autism has EXPLODED in being so common it’s crazy.
It is quite obvious. So no. This “autism diagnoses was broadened so now it’s common” hypothesis is fiction.
And, there are a number of excellent studies that show the dangers of this terribly aggressive vaccination schedule, worsened since 1990, as autism has exploded even more…and the myth of Reye’s Syndrome that resulted in switching away from baby aspirin…
…there are excellent studies showing that pregnant moms, and small children, exposed to acetominiphen have alarmingly larger odds of bearing an autistic child or becoming autistic, respectively.
The Reye’s Syndrome thing was a myth to begin with. And acetominoephen (paracetomol) affects the endocannabinoid system and in the earliest years of life, this system helps lay in the proper neural guiderails for the growth of the brain. This is precisely where autism seems to reside in the brain.
The fact that this comes from a president who is wildly unpopular with half the USA doesn’t mean it’s wrong.
I am the mother of a 21-year-old son who is autistic. I remember distinctly that my doctor told me that I could use Tylenol during all three of my pregnancies, but to use it judiciously. Of course, I wonder if there is something that I could have done to prevent this. The frustrating thing is that no one REALLY knows. I have followed Dr. Makary and Dr. Battacharya extensively since they began their positions at the FDA and NIH. I am incredibly interested in their commitment (I hope that they are still committed) to revisit studies and look into root causes that may be contributing to the increased diagnosis of autism. As they have discussed many times, addressing the gut microbiome and inflammation could be a promising approach. I fear that one day we truly may find a cause or a substantial contributing factor, and because the 'wrong team' made the discovery, 50% of us will not believe it.
My 25-year-old daughter has ADHD and dyslexia. She worked with an educational psychologist during her K-12 years, and we were told repeatedly that she is technically on the autism spectrum. I do not at all consider her to have autism when compared to my son. I believe that these numbers are overstated to increase fear. Maybe we also need to revisit what we define as autism.