
Hyponatremia, Observational Studies, and Changing Practice
as well as a whole lot of footnotes

For 25 years, I taught a class to our 4th-year medical students, Critical Appraisal of the Landmark Medical Literature (CALML). I loved teaching this course.
The idea behind the course was this: By the time a medical student reaches her senior year, her medical knowledge has come from textbooks, review articles, and lectures. From that point forward, however, continuing medical education depends on the ability to learn from the cases and to assimilate new data as it appears in the medical literature. CALML was meant to refine students’ skills in this type of learning.
I also hoped the course would provide a foundation in the medical literature by reviewing key studies. The syllabus for the course included an index of “landmark articles.” These were articles people frequently referenced, should be referencing, or were great for teaching critical appraisal. I edited the list every year, adding articles that students had presented and ones I had come across.1
When I read, Sodium Correction Rates and Associated Outcomes Among Patients With Severe Hyponatremia: A Retrospective Cohort Study, I thought, “Now this is an article I would have added to the syllabus.” We discussed it on This Fortnite in Medicine XXI, but I wanted one more say about it.
Background
Not a week goes by on a general medicine service that someone isn’t admitted with hyponatremia. The differential usually includes heart failure, cirrhosis, and SIADH, with some kidney disease and potomania thrown in for good measure. Any internist worth her salt will excitedly retreat to the whiteboard, calculate sodium and fluid needs, and design the fluid and electrolyte resuscitation.2 Repleting the sodium slowly means the patient spends more time in the hospital (and if it is really low, more time at risk of seizure). Repleting the sodium rapidly increases the risk of osmotic demyelination syndrome (ODS).3 What is interesting about these two competing outcomes is that the former is kind of the fault of the disease, while the latter is kind of the fault of the doctor. Hence, the chagrin factor for ODS is higher than for a prolonged, complicated hospitalization.
Design
The Annals article was impressive. It is a retrospective cohort study done at 21 hospitals over 15 years. Patients hospitalized with a serum sodium under 120 mEq/L were included. The exposure was the maximum 24-hour rate of sodium correction: slow (< 8 mEq/L), medium (8-12 mEq/L), or fast (> 12 mEq/L). The endpoint was a composite of 90-day death or delayed neurologic events (from 3-90 days). This is a perfect endpoint as it includes the negative outcomes of going too fast or too slow.
Results
Almost 14,000 patients were analyzed in this study. About 6,000 patients were in the slow group, 3,600 in the medium group, and 2,500 in the fast group. 1,800 patients had missing data. The fast repletion group had lower initial mean sodium levels and more people with sodium levels < 115 mEq/L. The primary outcome occurred in 21% of the patients – this is a sick group. The primary results are shown in the table below.
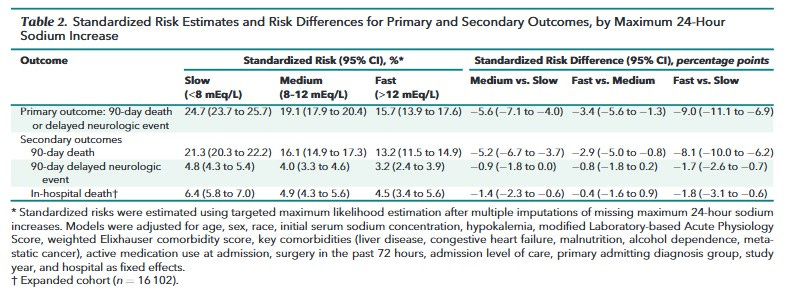
In short, the patients whose sodium returned to normal the fastest did best, though there was no statistical difference between the fast and medium groups. Demyelinating disease was exceedingly uncommon, accounting for < 1% of outcomes in each group. There were no subgroups in which the faster groups did worse.
Analysis
There are two ways of interpreting this data. First, it might be a true positive, indicating that patients whose sodium is corrected more quickly do better. If this were true, it would be a great example of a medical reversal; a practice that we have embraced for years would be wrong. What would have driven our faulty therapy would have been our fear of doing harm. This might be similar to years of withholding seizure medications, which we later learned were safe, in pregnant women.
This study could also be a false positive, probably due to confounding. Because this was an observational study, the patients in the three groups differed by far more than how quickly their sodium was repleted. Doctors who repleted sodium faster were different from those who went slow. As shown in Table 1, patients who had their sodium repleted faster received different medications. Thus, it might not have been the rapid sodium correction that helped the patients but the rest of their care. The patients themselves were also different. We might not be comparing a strategy of rapid vs. slow correction, but patients who rapidly correct themselves vs. those who slowly correct.4 As they always say, the smartest nephrologist knows less than the dumbest kidney.
The authors made extensive adjustments, but residual confounding remains possible. We know that only about 80% of observational studies predict the results of RCTs of the same question. Which brings us to what we do with this study. These results certainly open the door for an RCT comparing strategies of repleting sodium in patients with hyponatremia. A study published in the NEJM of patients with mild hyponatremia suggests that a future RCT of treatments for severe hyponatremia will give similar results as this observational study.
What do with patients now? It is a tough question. On the one hand, we should not change care based on observational studies. On the other hand, our standard of care is probably based more on tradition — and the worry about causing harm — than on treating patients the right way.
As one of the occasional gifts to our paying subscribers, a link to the final version of the article list appears below the paywall. It’s kind of long, 8-pages, but an interesting browse. Also, if you ever want to teach a course like CALML, drop me a note; I’d be happy to help.
See what I did there?
Formally known as central pontine myelinolysis.
Andrew made this point really well on the podcast.
Photo Credit: Sifan Liu
Keep reading with a 7-day free trial
Subscribe to Sensible Medicine to keep reading this post and get 7 days of free access to the full post archives.