
Recent News Headlines Imply that Cannabis is Deadly
The Study of the Week analyzes a study on cannabis use disorder.i The sample size is in the millions. But there are lots of limitations. Causality is a high bar.

Let’s talk today about a study that assess the risk of death after a hospital visit for cannabis use disorder or CUD.
JAMA Network Open published the Canadian study involving the entire population of Ontario Canada.

Cannabis use disorder is obviously an important public health topic. Cannabis use is increasing and there is a lack of causal studies proving its efficacy (for anything) or its safety. What’s more, the potency of cannabis is also rising. The drug clearly exerts effects on brain function. That’s why people use it.
As background, cannabis is remarkable because of its high therapeutic window. Therapeutic window is the difference between an effective dose and toxic dose. Warfarin and digoxin are classic cases of narrow therapeutic windows. You can easily cause harm with these drugs as even slightly high doses cause complications. Cannabis, however, is almost never deadly with acute consumption even in high doses.
This is not to say cannabis is “safe.” I put safe in quotes because the noun safe is always graded on a relative scale. Safe as in relative to not using cannabis or using it in low doses or comparing it to other legal substances, like alcohol.
There are many previous studies associating chronic and acute cannabis use with poor outcomes. The Canadian authors seek causation.
Let’s do the study first, then think about causation vs correlation.
The study The Ottawa-led team assessed the risk of death in the 5 years after a hospital visit for cannabis use disorder. They included all individuals who used the province’s public health insurance program—which covers 97% of residents between 2006 and 2021.
They used codes to find those who had a visit for CUD. Then matched them with 4 age and sex-matched people without CUD. Then they compared death rates in the next 5 years. This required serious efforts at matching. That sentence just sits there, and it’s easy to gloss over, but it is the core issue of the study.
(I will use rounded numbers.)
Step 1: about 100,000 people of 11 million had a hospital visit for CUD over the time period. That’s about 0.9%.
Step 2: these 100,000 were then matched to 400,000 age-and sex-matched people who were from the general population. They also matched to people admitted to the hospital for other drug-use conditions—stimulants, opioid and alcohol. So there were two comparisons.
Step 3: Obviously, the two groups are quite different. The authors did their best to match patients on things like socioeconomic status, medical conditions and other mental health conditions.
Step 4: The main comparisons. After adjustment, those who had a hospital encounter for CUD had a 2.8-fold greater risk of death in the five years compared with the general population. Actual hazard ratio was 2.79; 95% CI 2.62+2.97. The types of death that were elevated included suicide (10x), trauma (5x), opioid poisoning (5x) and lung cancer (4x).
Step 5: Comparison to other drug-abuse hospital encounter. This is best shown in the image. Notably, of all the drug-use encounters, CUD had the lowest five-year risk.

The authors concluded that this was a “markedly” increased risk.
“These findings suggest important clinical and policy implications, given global trends toward cannabis legalization and market commercialization accompanied by increasing cannabis use and CUDs.”
The accompanying editorialists agreed.
“…the current evidence is enough to sound an alarm; cannabis is addictive; cannabis use disorder is on the rise; and those affected by cannabis use disorder are at an increased risk of premature death.”
My Comments:
Both authors and editorialists use causal language. These findings suggest…Or: Those affected by CUD are at increased risk of death…
I harbor no judgements about cannabis. Whether it has proven efficacy for things like nausea, insomnia, or chemotherapy induced anorexia will require randomized placebo-controlled trials.
My point today is to refute the notion that this study proves cannabis kills. This column is less about cannabis and more about using studies to make conclusions.
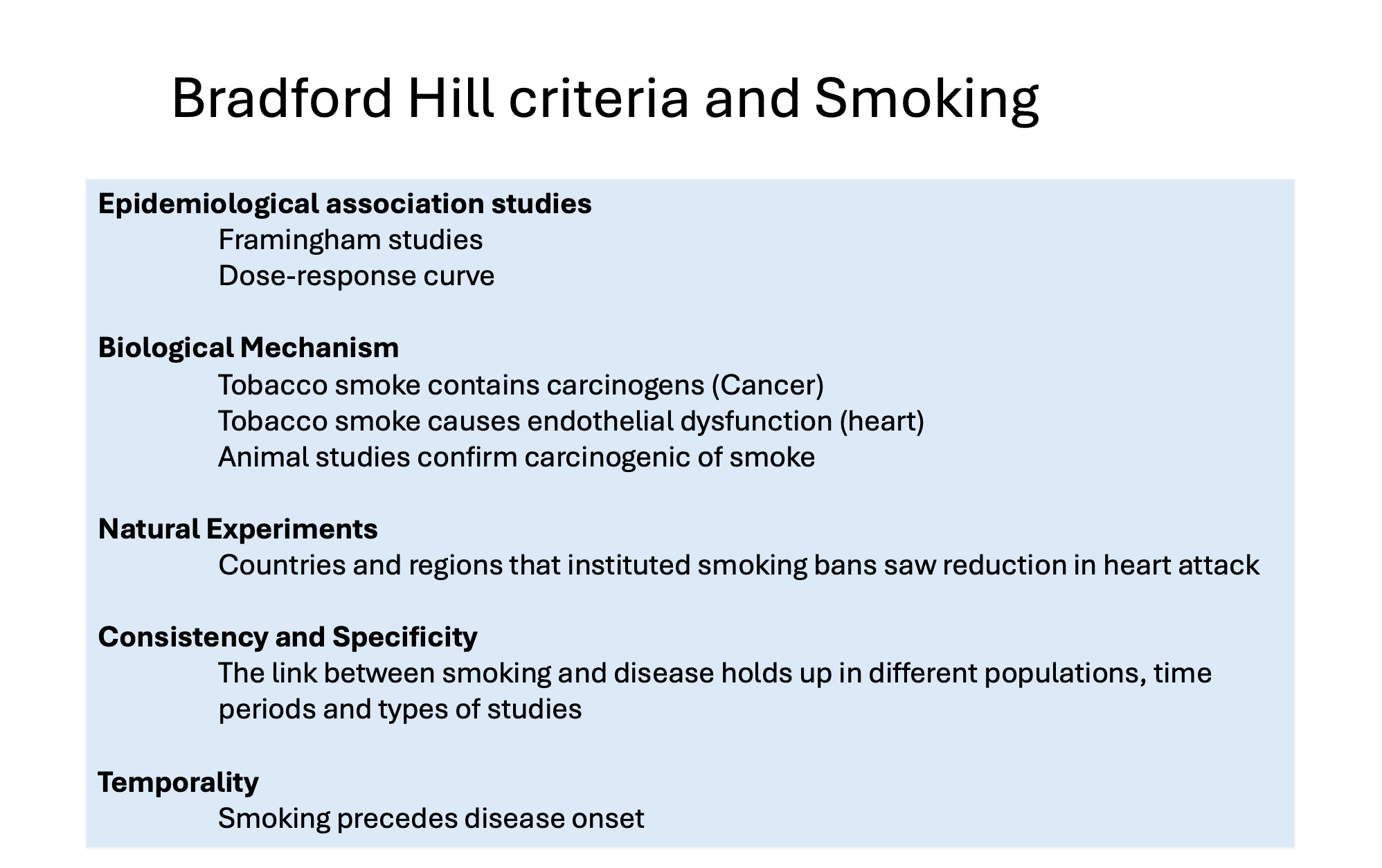
As an exercise in causal inference, we should consider how smoking was proven to cause cancer and heart disease. This required more than simple association studies. I made a slide of the causal proof for smoking.
This study offers only one line of evidence—that of an association of CUD and higher rates of death. Plus, this is a profoundly weak association study.
Three reasons why you should put little weight in this study. The authors listed many of these limitations in the discussion section.
First, there is almost certain confounding bias. That is, people who have a hospital encounter for CUD surely have other conditions that could reduce survival. The authors attempt to match them to similar types of people, but this is near impossible with only health record data. This is a fatal flaw because it makes it impossible to know whether it was the cannabis or something else.
The second problem was the comparison. Instead of comparing to a group of patients who had a hospital encounter, they matched to the general population. When comparing against people who present for other drug use disorders, CUD looks least deadly. Had this been the primary comparison, the headlines would be totally different.
Finally, I remind you about one of the most important papers covered on Sensible Medicine. This was the work of Dena Zeraatkar, and colleagues from McMaster who showed that there are literally a quadrillion different ways to analyze such big data. Crucially, these choices can determine whether a study finds a positive or negative association. The Canadian authors made one analytic choice in their analysis—which is typical. But what if they made other choices?
Final conclusion:
It’s sad that we have not had randomized placebo controlled trials of cannabis. These would help sort out efficacy and safety for specific conditions. An RCT balances the two groups for both known and unknown factors. Then you can make causal inference.
To infer causation of harm from cannabis, especially mortality, will take a lot more and varied form of evidence—as outlined initially by Bradford Hill.
I don’t think cannabis, especially at high doses is “healthy,” but before we start calling it deadly, we ought to have proper evidence.
Because making outsized conclusions from weak evidence shreds trust in the medical profession.
Thanks for posting an excellent ejaculation of solid warning points regarding out-of-control (no pun here) publication of observational studies that -- no matter how large -- remain badly tainted by all kinds of poisoning flaws and disabling "technical issues". How unfortunate that the Talking Heads of Cable TV (i.e. the highly paid news folks with the hair spray, the constant smiles, and bleached teeth) regularly regurgitate 24/7 their blizzards of buzzwords while spewing and gushing over the "crap science" like the present study from Canada. . . . . and thus mislead badly many of us out here in 'Murika --- unwashed yokels, confused hicks, and even the odoriferous hill-billy folks sitting on their ramshackle porches, sipping moonshine, surfing the Internet with Mac laptops, and occasionally petting their old, overweight, faithful coon hounds who perch nearby, snoring and dreaming and farting.
Thanks for another example of the hazards of suggesting causality in observational research. A pretty well described Cannabis Hyperemesis Syndrome exists in which usually heavy users present with intractable nausea and vomiting. I care for these patients not infrequently and the clear recommendation is to cut back or abstain from heavy intake. Much remains unknown about the health consequences of high volume users but hopefully we can get some RCT’s done and get some better understanding.