
The Most Important Trial in Modern Cardiology
Chapter 3 of our coronary artery disease mini-series explores the ISCHEMIA trial

In Chapter 1 of this mini-series, I explained the disruption wrought by the COURAGE trial. Seriously? Stenting severe coronary lesions did not improve survival over simple tablets?
Chapter 2 added to the oodles of studies showing how much doctors can be fooled by the placebo effect. The ORBITA trial demonstrated that the caring signal of placing a stent is massive.
I am super-excited to show you the ISCHEMIA trial. It’s good science. And it puts to the test an everyday practice in US cardiology.

Modern cardiology does a lot of things, but highest on its goals is the search for ischemia. Ischemia is medical jargon for finding obstructions in coronary arteries. These lead to an inadequate blood supply to the heart muscle. We call this athero-sclerosis, or hardening of the arteries.
The grand idea is an offshoot of the clogged pipe notion of coronary artery disease. We should find and then “fix” a widow-maker before it occludes and causes a heart attack or sudden death.
ISCHEMIA trialists conceived the study to resolve two areas of uncertainties.
First was to resolve the main weakness of COURAGE: that it randomized patients after the angiogram. Skeptics argued—rightly perhaps—that doctors did not allow the most worrisome patients in the trial. And that is what explains the lack of survival benefit from the intervention. ISCHEMIA resolved this issue by randomizing patients before the angiogram.
The second area of uncertainty was the question of going right to the cath lab for angiography after a positive stress test. ISCHEMIA tested this question by randomizing two strategies: one was the standard go to the cath lab if the stress is positive, and the other was a delayed or conservative strategy wherein patients were treated with medial therapy and angiograms were done only for recurrent symptoms.
ISCHEMIA, therefore, was not a stent vs medicine trial. It was a conservative vs early invasive approach to ischemia test.
The Trial
Patients had to have a positive stress test. And it had to be seriously positive. The cutoff was greater than 10% of the heart ischemic. (People argue that it wasn’t enough ischemia, but I would emphasize that nearly all such positive stress tests go to angiography).
One other important nuance was that a blinded coronary CT scan was done before randomization to a) make sure there was coronary disease (not just a positive stress test) and b) exclude left main coronary artery disease.
About 2600 patients were randomized in each of the two groups. Average age 64 years. Nearly half of these patients had ≥ 3-vessel disease. (Which eliminates the argument that the trial enrolled patients with mild disease.)
The primary endpoint was a composite of 5 bad things: death due to cardiovascular causes, MI, unstable angina, heart failure, or resuscitated cardiac arrest.
Here was the result. After a median follow-up of 3.2 years the hazard ratio was 0.93. Confidence intervals 0.80-1.08. This did not reach statistical significance.
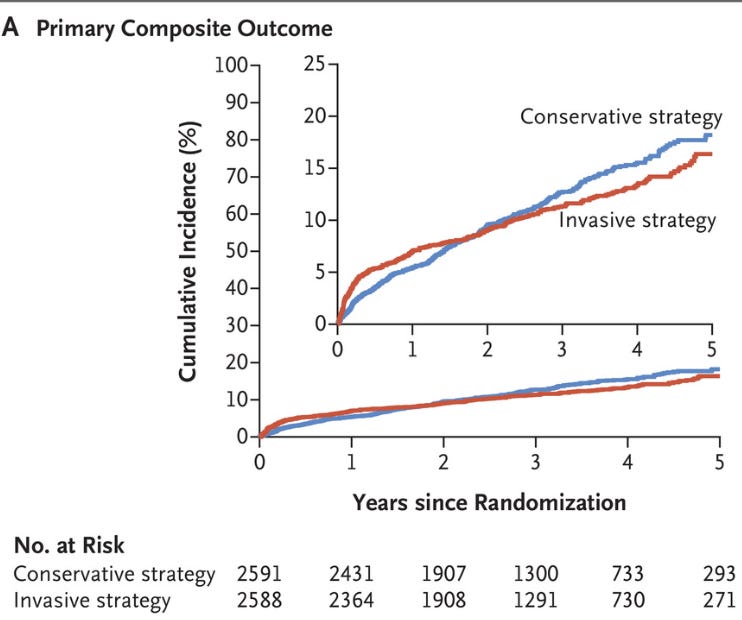
Cardiovascular death or MI did not differ significantly. Rates of all-cause death were nearly identical. There was no subgroup that seemed to benefit more or less. Importantly, the subgroup with the most severe disease did not benefit from the early invasive strategy.
Here are two key images from the supplement. It shows how many (actually how few) patients in the delayed or conservative strategy actually went on to have a cath or revascularization (either a stent of bypass).
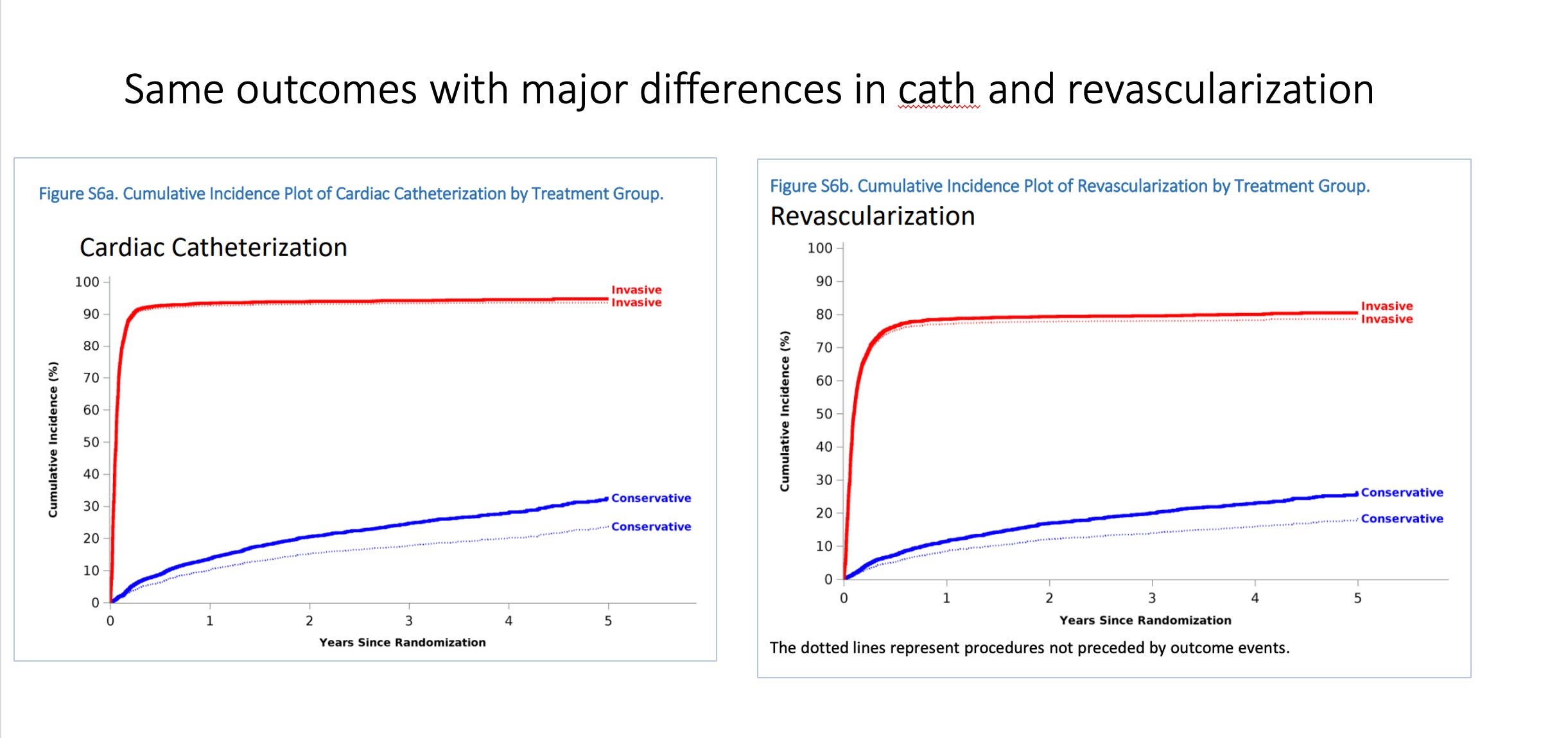
To me, these figures are super-important. They say that patients with positive stress tests, many of whom had severe multi-vessel coronary artery disease, achieved the same rate of events with nearly 70% fewer procedures.
Other findings: ISCHEMIA trialists also collected data on angina. As expected the invasive arm looked better. But the trial was not blinded—and ORBITA showed how important that was.
Comments:
If you delve into the details, you will see commentaries about the curves crossing—early harm from the invasive strategy and then benefit. You will here talk about the definition of MI. And about the intensity of medical therapy.
These are distractions to the main finding: that in patients with positive stress tests, nearly all of whom would now go straight to the cath lab, there was no substantial difference in outcomes at more than three years.
The one caveat that is important is the blinded coronary angiogram. This increased the safety and internal validity of the trial. But it diminished its external validity.
Translation: by excluding patients without CAD, it enhances our confidence in the findings (internal validity). By excluding patients with left main disease, it satisfied a safety/ethical standard of not treating patients with left main disease medically.
But it puts a clinician who wants to use this data into a bind. Because. In real life, you don’t know if a positive stress test will turn out to have left main disease. There is a low chance, but missing left main disease is problematic. Here is what Sanjay Kaul, Andrew Foy, and I wrote in an academic review.
ISCHEMIA surely upends the knee-jerk thinking that positive stress tests require a cath. A conservative strategy of medical therapy with cath reserved for symptoms should probably be favored. (Perhaps with a coronary angiogram—for the purists.)
I am drawn most to what this trial says about our scientific understanding of atherosclerotic heart disease. ISCHEMIA strongly supports the idea that atherosclerotic disease is a systemic disease that requires systemic therapy (lifestyle and medical therapy). Yes. We diagnose partial blockages, but these are simply focal manifestations of the systemic disease.
The challenge to this idea is that people think, wait, wait, we’ve seen stents save lives in the setting of MI, why would it would be different in the chronic stable situation?
It’s different because treatment of sick people is always different from prevention. When these partial blockages are just there (stable), we don’t know that they will fracture and cause MI. ISCHEMIA confirms COURAGE, and the many other similar studies that find preventive stents don’t improve outcomes over medical therapy.
The next question, the harder question, the truly existential question for cardiology, is: if there is no advantage to the early invasive approach to treating ischemia, why should we be searching for it in the first place?
Why not encourage positive lifestyles, and use medical therapy, like statins, and reserve revascularization for patients with refractory symptoms. That would mean a lot less stress tests and angiograms and stents.
Three years on from ISCHEMIA, I haven’t seen much of a change. It might take a generation or so to upend the clogged pipe frame of cardiology.
JMM
Next week, I will tell you about another utterly surprising trial. I can’t wait. Thanks again for your support.
You do such a wonderful job of explaining medical jargon in simple terms, Dr. M. If all cardiologists would do the same with each patient in this situation, it would lead to truly informed shared decision making. It would probably be even better if a diverse cardiology team were involved (see link below). As my PCP told me years ago when referring me to a non-surgical orthopedist first, he said if I went to a surgeon first, the recommendation would no doubt be surgery because when you have a hammer, everything looks like a nail. As an aside, in addition to the placebo effect, I wonder if learning you have clogged arteries leads to greater changes in behavior? It would scare the bejesus out of me!
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1440300/
There are fifteen studies that prove opening arteries provides no benefit for people with stable angina beyond that provided by optimal medical therapy alone. Our entire system is still designed to find blockages and open them and very few patients receive best practice medical treatment. That is part of the reason that our health care costs twice as much and citizens of other developed countries live longer. Optimal medical therapy first is the way they do business in Great Britain. It is all about the money in the US. Use your influence to change our system so that we treat chronic diseases more effectively.
https://www.ajmc.com/view/aug08-3509p521-528